

Evidence-based decision making for malaria elimination applying the Freedom From Infection statistical framework in five malaria eliminating countries: an observational study
- PMID: 40845885
- PMCID: PMC12368415
- DOI: 10.1016/S2214-109X(25)00236-0
Evidence-based decision making for malaria elimination applying the Freedom From Infection statistical framework in five malaria eliminating countries: an observational study
Abstract
Background: Routine surveillance is a pillar of malaria programmes, and the primary source of data used for decision making. However, any inference when relying on routine data to inform decision making is limited by how effective the system is at measuring the actual malaria burden. Here, we aimed to extend the Freedom From Infection (FFI) framework to produce species-specific estimates of surveillance system sensitivity and probability of freedom from malaria, combine multiple surveillance components including community case management and active case detection, and apply the FFI model in five malaria eliminating settings.
Methods: Monthly routine data on Plasmodium falciparum and Plasmodium vivax and health system factors were collected from 1515 facilities across five countries. Additionally, data from 12 community health workers and from 10 767 individuals from cross-sectional surveys (active case detection) were available. The data were analysed using FFI models accounting for multiple malaria species and surveillance components. The primary outcomes were the sensitivity of the surveillance system and the probability of malaria freedom.
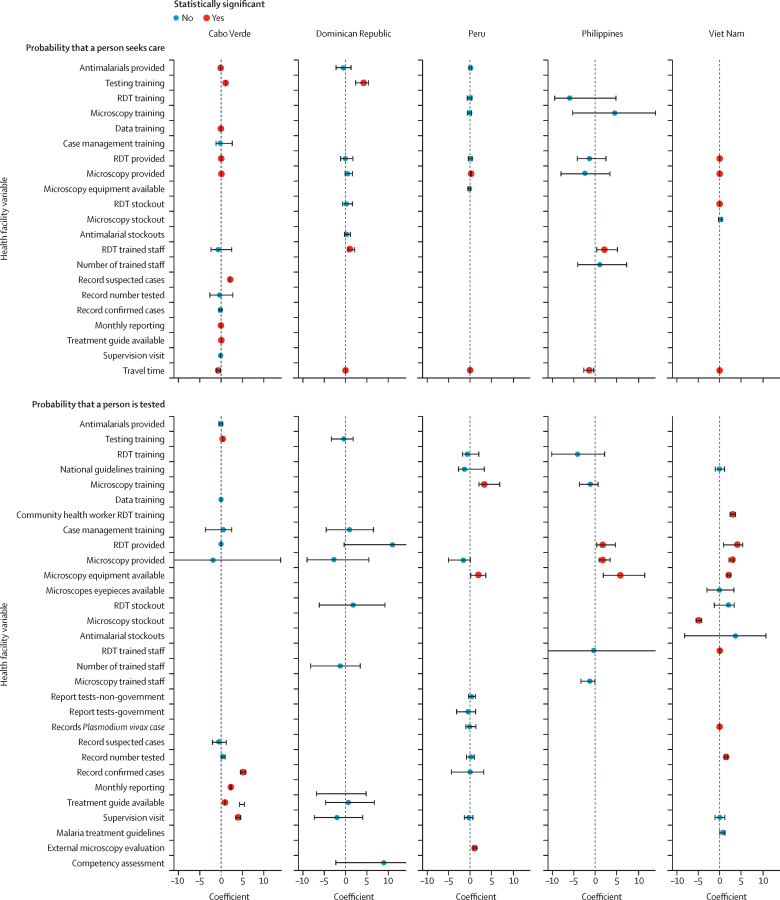
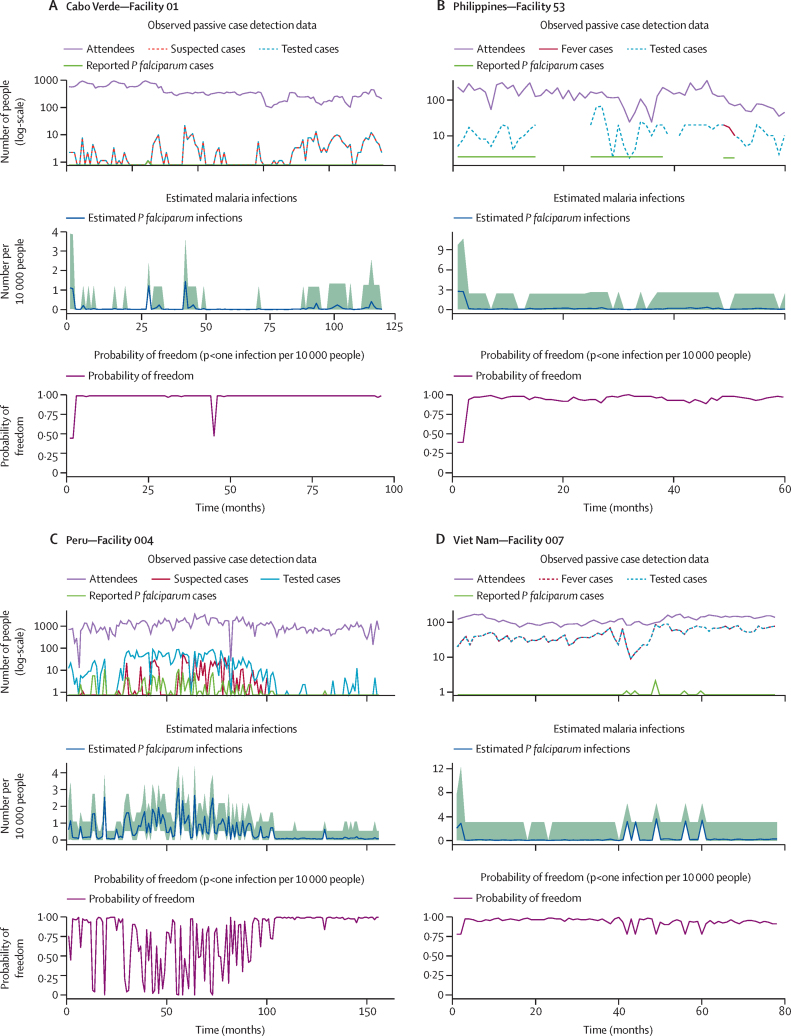
Findings: Strong surveillance systems were characterised by access to testing and treatment supplies, training on diagnostics and case management within the previous 12 months, and shorter estimated travel times to facilities. Only half of the facilities (841 of 1515 facilities for P falciparum and 771 of 1455 facilities for P vivax) had sufficient sensitivity to achieve and maintain a high probability of freedom, consistent with having achieved malaria elimination, with either passive case detection data alone or when combined with active case detection.
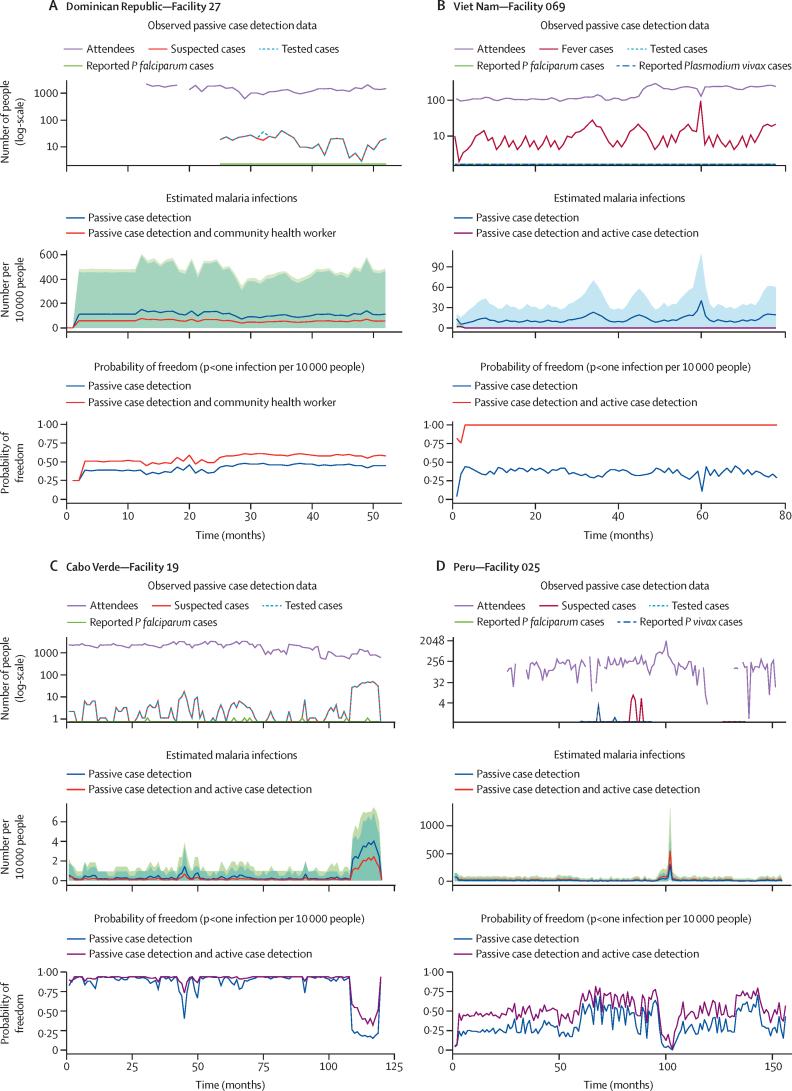
Interpretation: Applying the FFI model framework to malaria surveillance data can provide programmes with information to support decision making, specific to malaria species. When routine malaria surveillance systems are strong, they are sufficient to achieve and maintain a high probability of freedom. Including additional surveillance components such as community case management and active case detection with multiple diagnostic tools can help improve estimates for which routine malaria data alone are not sufficient to ensure confidence in elimination.
Funding: The Bill and Melinda Gates Foundation, the Global Institute for Disease Elimination, and the Carter Center.
Copyright © 2025 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures


References
-
- WHO . World Health Organization; Geneva, Switzerland: 2018. Malaria surveillance, monitoring & evaluation: a reference manual.
-
- WHO . World Health Organization; Geneva, Switzerland: 2024. World malaria report 2024: addressing inequality in the global malaria response.
-
- WHO . World Health Organization; Geneva, Switzerland: 2020. Preparing for certification of malaria elimination.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
