

Trapeziectomy and Ligament Reconstruction Using a Reinforced Half-Slip of the Extensor Carpi Radialis Longus Tendon for Thumb Carpometacarpal Osteoarthritis
- PMID: 40851845
- PMCID: PMC12367041
- DOI: 10.2106/JBJS.OA.25.00147
Trapeziectomy and Ligament Reconstruction Using a Reinforced Half-Slip of the Extensor Carpi Radialis Longus Tendon for Thumb Carpometacarpal Osteoarthritis
Abstract
Background: Carpometacarpal (CM) joint osteoarthritis of the thumb is characterized by pain and impaired thumb function in terms of pinch and range of motion. Here, we newly adopted a trapeziectomy with a graft-augmented ligament reconstruction procedure, in which the reconstructed ligament is reinforced using a half-slip extensor carpi radialis longus (ECRL) tendon.
Methods: From 2015 to 2022, 101 hands of 95 patients with CM joint osteoarthritis of the thumb underwent trapeziectomy with graft-augmented ligament reconstruction using the half-slip ECRL tendon to reconstruct the ligament. The reconstructed ligament was reinforced by wrapping 3 times with the half-slip ECRL tendon. All patients underwent a 1-year assessment, and 29 hands of 26 patients were followed up for >4 years postoperatively.
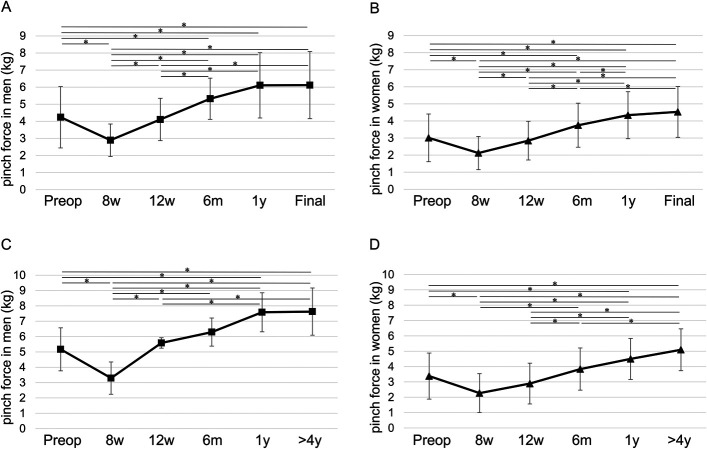
Results: Motion pain, as assessed by visual analogue scale, was significantly improved from 56.9 ± 20.6 preoperatively to 4.2 ± 10.1 at the 1-year assessment (p < 0.001). Radial and palmar abduction also increased significantly from 46.0° ± 11.0° and 49.7° ± 8.8° preoperatively, respectively, to 58.4° ± 6.4° (p < 0.001) and 59.5° ± 6.3° (p < 0.001), respectively, at 12 months postoperatively. Both male and female tip pinch increased significantly from 4.2 ± 1.8 and 3.0 ± 1.4 preoperatively, respectively, to 6.1 ± 1.9 (p = 0.002) and 4.3 ± 1.4 (p < 0.001) at the 1-year postoperative evaluation. We observed no impingement of the first metacarpal and scaphoid bones due to sinking of the first metacarpal bone, and repeat surgery due to rupture of the reconstructed ligament or fractures at the bone hole, was not needed for the 101 hands followed for approximately 1 year and the 29 hands followed over 4 years.
Conclusions: Trapeziectomy combined with graft-augmented ligament reconstruction, using a reinforced half-slip ECRL tendon wrapped 3 times, may serve as an effective treatment option for primary thumb carpometacarpal osteoarthritis. This approach offers significant pain relief, improved range of motion and pinch strength, and prevents postoperative impingement of the first metacarpal across all Eaton stages in the short - medium term.
Level of evidence: Therapeutic Level Ⅳ. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2025 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A881).
Figures





References
-
- Hattori Y, Doi K, Dormitorio B, Sakamoto S. Arthrodesis for primary osteoarthritis of the trapeziometacarpal joint in elderly patients. J Hand Surg. 2016;41(7):753-9. - PubMed
-
- Fulton DB, Stern PJ. Trapeziometacarpal arthrodesis in primary osteoarthritis: a minimum two-year follow-up study. J Hand Surg. 2001;26(1):109-14. - PubMed
-
- Rizzo M, Moran SL, Shin AY. Long-term outcomes of trapeziometacarpal arthrodesis in the management of trapeziometacarpal arthritis. J Hand Surg. 2009;34(1):20-6. - PubMed
-
- Huang K, Hollevoet N, Giddins G. Thumb carpometacarpal joint total arthroplasty: a systematic review. J Hand Surg Eur. 2015;40(4):338-50. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials