

Comparative Analysis of Bite Force after Cranioplasty with and without Temporalis Dissection in Large Skull Defects Caused by Decompressive Craniectomy
- PMID: 40852068
- PMCID: PMC12370351
- DOI: 10.1055/s-0045-1809047
Comparative Analysis of Bite Force after Cranioplasty with and without Temporalis Dissection in Large Skull Defects Caused by Decompressive Craniectomy
Abstract
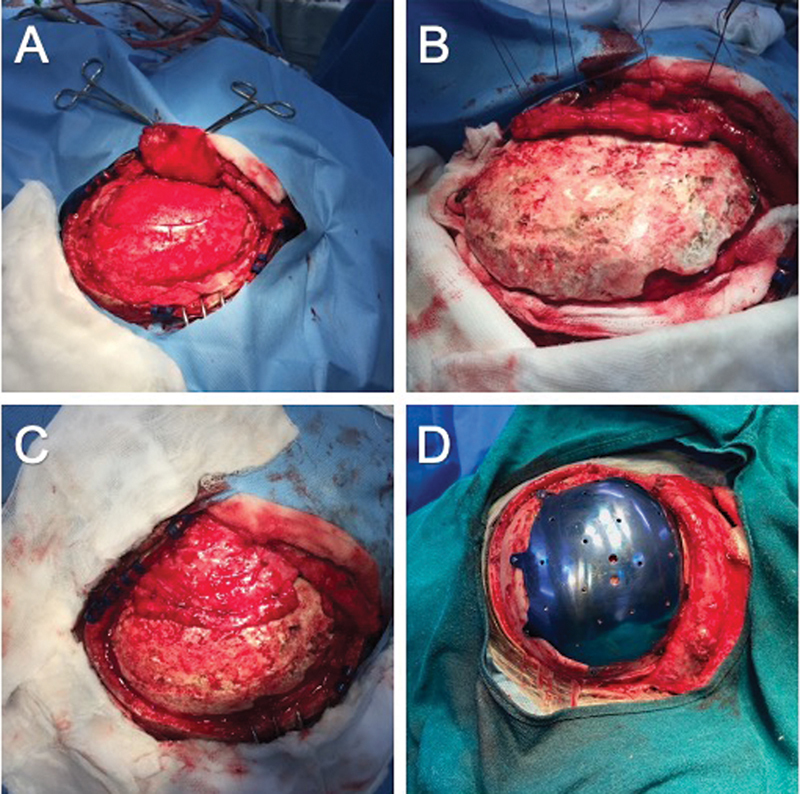
Introduction: Cranioplasty involves repairing the skull defect using an autologous bone flap or synthetic molds. The temporalis muscle, detached during decompressive craniectomy (DC), may be reattached to the bone flap for better cosmetic reconstruction. Along with the masseter and pterygoid muscles, the temporalis muscle significantly contributes to the human bite force. In this study, we analyze patients' bite force in which the temporalis muscle was either dissected and reattached or left undisturbed during cranioplasty.
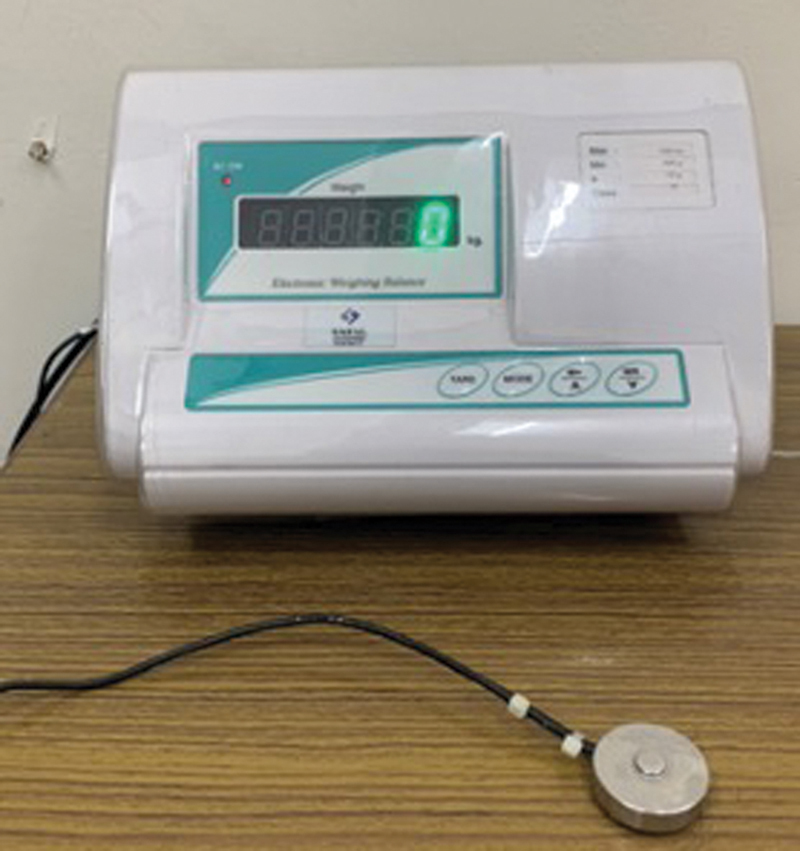
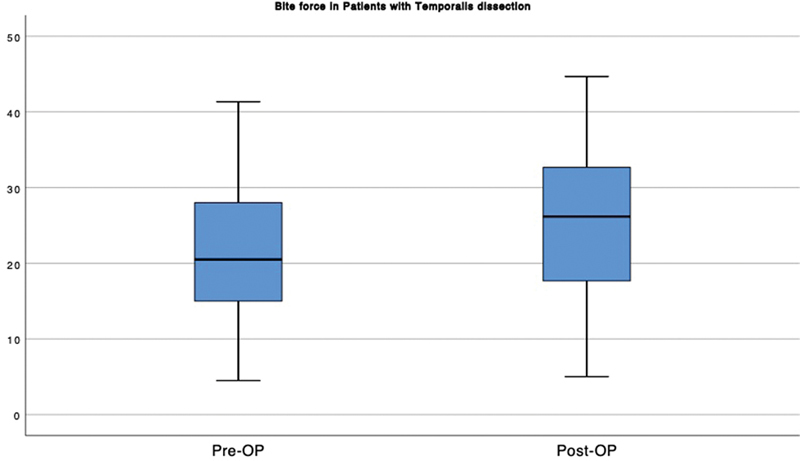
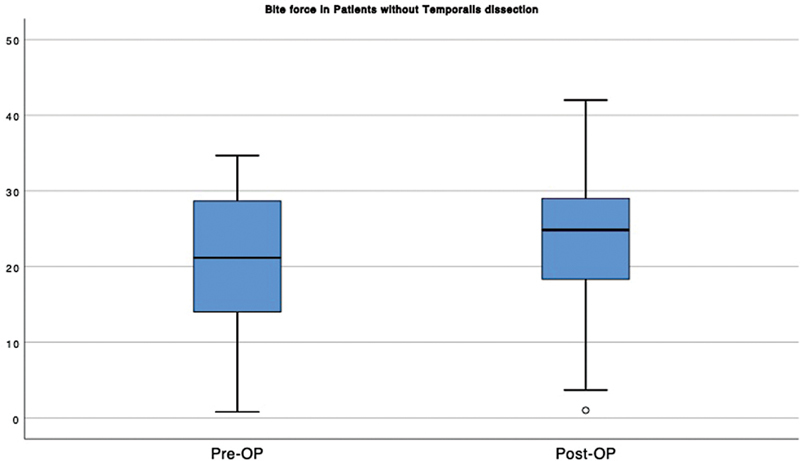
Materials and methods: All patients who previously underwent DC for traumatic brain injury or stroke were grouped into two, depending on the method of cranioplasty. In group 1, patients underwent temporalis muscle dissection and reattachment to the bone flap or prosthesis. In group 2, the temporalis muscle was left undisturbed. The bite force of the subjects was measured bilaterally in both groups by a gnathodynamometer before cranioplasty and 3 months after the surgery. We compared the difference in bite force of the subjects individually on both sides, preoperatively and postoperatively, as well as between the groups.
Results: This study included 36 patients over 18 years of age, with 18 patients in each group. Preoperatively, the bite force of all the subjects was decreased on the side of the DC compared with the normal side. After cranioplasty, the bite force significantly improved compared with preoperative values in both groups.
Conclusion: Temporalis dissection can be safely done during cranioplasty. There is improvement in bite force after cranioplasty with or without temporalis dissection.
Keywords: bite force; cranioplasty; decompressive craniectomy; temporalis dissection.
Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Outcomes of cranioplasty following decompressive craniectomy in the pediatric population.J Neurosurg Pediatr. 2013 Aug;12(2):120-5. doi: 10.3171/2013.4.PEDS12605. Epub 2013 Jun 21. J Neurosurg Pediatr. 2013. PMID: 23790219
-
Morphological, functional and neurological outcomes of craniectomy versus cranial vault remodeling for isolated nonsyndromic synostosis of the sagittal suture: a systematic review.JBI Database System Rev Implement Rep. 2015 Sep;13(9):309-68. doi: 10.11124/jbisrir-2015-2470. JBI Database System Rev Implement Rep. 2015. PMID: 26470674
-
A systematic review and meta-analysis of factors involved in bone flap resorption after decompressive craniectomy.Neurosurg Rev. 2022 Jun;45(3):1915-1922. doi: 10.1007/s10143-022-01737-z. Epub 2022 Jan 21. Neurosurg Rev. 2022. PMID: 35061139
-
Characteristics and Clinical Significance of Skull Defect Restoration in Young Patients: A Single-center Report and Literature Review.J Craniofac Surg. 2025 Jul-Aug 01;36(5):1655-1660. doi: 10.1097/SCS.0000000000010851. Epub 2024 Nov 11. J Craniofac Surg. 2025. PMID: 39527727
References
-
- Lin J, Frontera J A. Decompressive hemicraniectomy for large hemispheric strokes. Stroke. 2021;52(04):1500–1510. - PubMed
LinkOut - more resources
Full Text Sources