

The Role of Mesenchymal Stromal Cells in the Treatment of Bronchopulmonary Dysplasia: A Multi-Prong Approach for a Heterogeneous Disease
- PMID: 40853849
- PMCID: PMC12377523
- DOI: 10.1002/cph4.70038
The Role of Mesenchymal Stromal Cells in the Treatment of Bronchopulmonary Dysplasia: A Multi-Prong Approach for a Heterogeneous Disease
Abstract
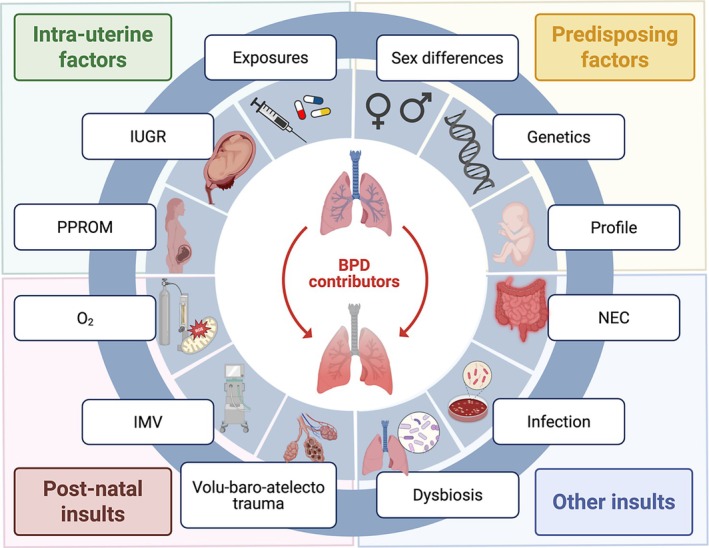
Acute lung injury can be a devastating ailment leading to death in patients of all ages. In preterm neonates, lung injury is unique and unlike what is seen in pediatric and adult populations. The physiology behind the acute lung injury endured in developing lungs and the chronicity of harmful stimuli vastly distinguish how bronchopulmonary dysplasia (BPD), the most common complication of prematurity, settles in as a chronic lung disease with lifetime sequelae. Despite being recognized for over 50 years, BPD continues to puzzle the world of neonatology with a shifting phenotype that parallels improvement in neonatal care. The improved understanding of BPD's far-reaching and long-term consequences on the lung and other organs highlights the need to find effective interventions, making it a priority of neonatal research. In this review, we provide an overview of BPD and its associated consequences. Then, we examine the biological premises for mesenchymal stromal cells as a promising therapy, reviewing current translational efforts, challenges, and future directions toward bringing mesenchymal stromal cell therapy to BPD patients.
© 2025 The Author(s). Comprehensive Physiology published by Wiley Periodicals LLC on behalf of American Physiological Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Systemic corticosteroid regimens for prevention of bronchopulmonary dysplasia in preterm infants.Cochrane Database Syst Rev. 2023 Mar 13;3(3):CD010941. doi: 10.1002/14651858.CD010941.pub3. Cochrane Database Syst Rev. 2023. PMID: 36912887 Free PMC article.
-
Early (< 8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants.Cochrane Database Syst Rev. 2017 Oct 24;10(10):CD001146. doi: 10.1002/14651858.CD001146.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2021 Oct 21;10:CD001146. doi: 10.1002/14651858.CD001146.pub6. PMID: 29063585 Free PMC article. Updated.
-
Delivery room interventions to prevent bronchopulmonary dysplasia in preterm infants: a protocol for a systematic review and network meta-analysis.BMJ Open. 2019 Aug 18;9(8):e028066. doi: 10.1136/bmjopen-2018-028066. BMJ Open. 2019. PMID: 31427322 Free PMC article.
-
Systemic corticosteroid regimens for prevention of bronchopulmonary dysplasia in preterm infants.Cochrane Database Syst Rev. 2017 Jan 31;1(1):CD010941. doi: 10.1002/14651858.CD010941.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Mar 13;3:CD010941. doi: 10.1002/14651858.CD010941.pub3. PMID: 28141913 Free PMC article. Updated.
References
-
- Abu Jawdeh, E. G. 2017. “Intermittent Hypoxemia in Preterm Infants: Etiology and Clinical Relevance.” NeoReviews 18, no. 11: e637–e646. 10.1542/neo.18-11-e637. - DOI
-
- Ahn, S. Y. , Chang Y. S., Kim J. H., Sung S. I., and Park W. S.. 2017. “Two‐Year Follow‐Up Outcomes of Premature Infants Enrolled in the Phase I Trial of Mesenchymal Stem Cells Transplantation for Bronchopulmonary Dysplasia.” Journal of Pediatrics 185: 49–54.e2. 10.1016/j.jpeds.2017.02.061. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
