

Narrative review of metabolic syndrome and its relationships with non-alcoholic fatty liver disease, gonadal dysfunction and obstructive sleep apnea
- PMID: 40855341
- PMCID: PMC12376488
- DOI: 10.1186/s13098-025-01903-5
Narrative review of metabolic syndrome and its relationships with non-alcoholic fatty liver disease, gonadal dysfunction and obstructive sleep apnea
Abstract
Background: Metabolic syndrome is an emerging health problem, and its prevalence is rapidly increasing. Therefore, we first aimed to investigate its pathophysiology, focusing on the insulin resistance state and the consumption of high-calorie diets. In addition, previous studies have shown an association between metabolic syndrome and non-alcoholic fatty liver disease, gonadal dysfunction and obstructive sleep apnea, but little is known about the nature of the relationship between metabolic syndrome and these conditions. Therefore, second, we aimed to investigate this relationship to better predict the risk of these diseases in MetS patients and vice versa.
Materials and methods: We conducted a comprehensive search in multiple scientific databases to examine the pathophysiology of metabolic syndrome and to investigate the nature of the relationship between metabolic syndrome and these conditions. The selection of the articles included in this review is based on their pertinence to the research issue, methodological rigor, and contribution to the field.
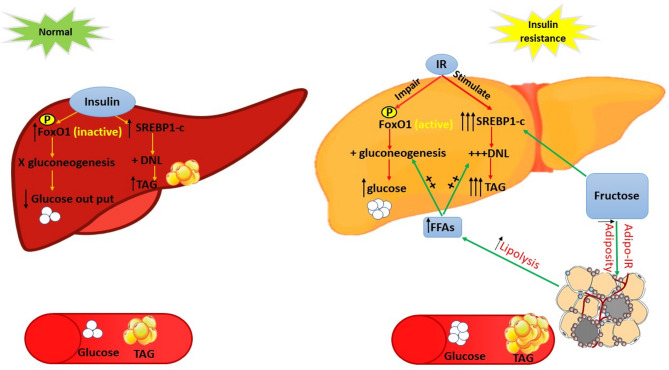
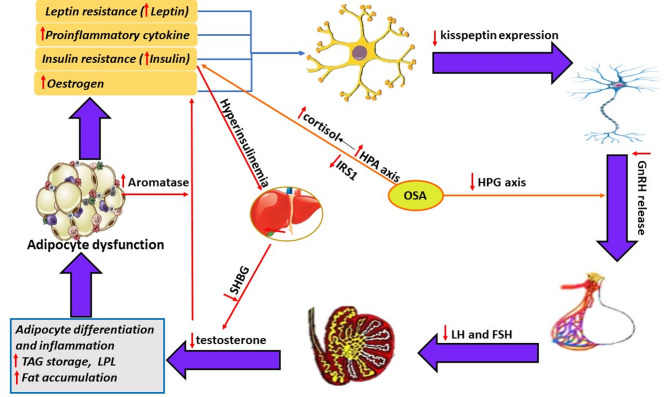
Results: This study revealed that insulin resistance and high fructose consumption are two important contributors to the pathophysiology of metabolic syndrome. Additionally, a bidirectional relationship was detected between metabolic syndrome and both non-alcoholic fatty liver disease and secondary male hypogonadism. Both non-alcoholic fatty liver disease and testosterone deficiency can lead to metabolic dysregulation and insulin resistance, which in turn exacerbate this clinical condition. A mutual relationship between metabolic syndrome and polycystic ovarian syndrome has been demonstrated, with similar risk factors and treatment strategies. Finally, an independent relationship was found between obstructive sleep apnea and the components of metabolic syndrome.
Conclusion: Metabolic syndrome is closely related to non-alcoholic fatty liver disease, gonadal dysfunction and obstructive sleep apnea. It is therefore recommended that further studies be conducted to better understand these relationships to develop a comprehensive treatment strategy for metabolic health and these conditions.
Keywords: Dyslipidemia; High caloric diet; Insulin resistance; Male hypogonadism; Metabolic syndrome; Non-alcoholic fatty liver disease; Obstructive sleep apnea; Polycystic ovarian syndrome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study does not involve human participants or animal use; therefore, ethical approval was not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Kylin E. Studies of the hypertension-hyperglycemia-hyperuricemia syndrome. Zentralbl Inn Med. 1923;44:105–27.
-
- Reaven GM. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595–607. - PubMed
-
- Kaplan NM. The deadly quartet: Upper-Body obesity, glucose intolerance, hypertriglyceridemia, and hypertension. Arch Intern Med. 1989;149(7):1514–20. - PubMed
-
- Alberti G. Introduction to the metabolic syndrome. Eur Heart J Supplements. 2005;7(supplD):D3–5.
-
- Reaven P. Metabolic syndrome. J Insur Med. 2004;36(2):132–42. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
