

Normalizing daily awakening and breathing coordination at 15 heterogenous ICUs: a multicenter post-implementation survey
- PMID: 40855450
- PMCID: PMC12376443
- DOI: 10.1186/s43058-025-00770-5
Normalizing daily awakening and breathing coordination at 15 heterogenous ICUs: a multicenter post-implementation survey
Abstract
Background: Despite high post-implementation adherence, clinicians may have unresolved questions or concerns regarding use of a protocol to standardize routine daily coordination of the spontaneous awakening trial (SAT) and spontaneous breathing trial (SBT) on ventilated patients. Unresolved questions or concerns may unwittingly curtail practice normalization, impacting practice sustainment when implementation support is withdrawn. The objective of this study was to identify unresolved questions or concerns that may persist following successful implementation of a coordinated SAT/SBT (C-SAT/SBT) protocol.
Methods: We used an attributed, cross-sectional survey of physicians, advanced practice providers, nurses and respiratory therapists likely to have participated in a C-SAT/SBT in 12 hospitals (15 intensive care units) in Utah and Idaho. We evaluated clinician perceptions of acceptability, including ease of use, usefulness and confidence, along with perceived practice normalization, six months post implementation of a protocol to routinize C-SAT/SBT use.
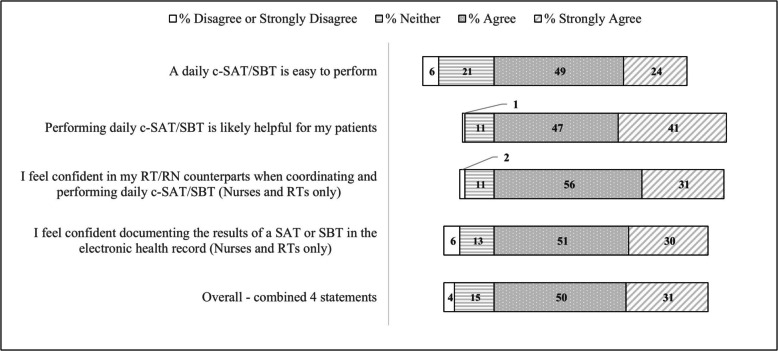
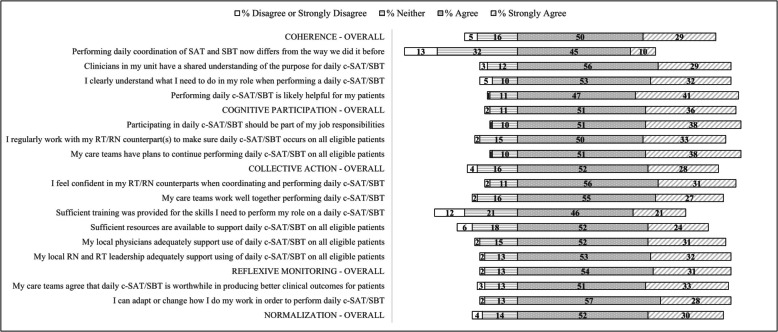
Results: C-SAT/SBT adherence was 83.1% at the 6th month post implementation. 606 clinicians completed the survey (response rate: 50.0%). Perceived individual usefulness, ease of use, and confidence using the C-SAT/SBT protocol were high [range: 72.1%-88.1% agree/strongly agree], though individuals not performing an SAT or SBT in more than six months and respiratory therapists scored lower. Perceived practice normalization was similar with 82.0% aggregate agreement [agree/strongly agree]. However, when stratifying respondents into four categories based upon respondent percentage agreement with all statements, 71% did not agree with at least one practice normalization statement and 27% agreed with less than 80% of statements, varying by role and site. Sets of observable characteristics or phenotypes regarding the degree of practice normalization begin to emerge by subgroup.
Conclusions: Unresolved questions or concerns may persist regarding implementation of a C-SAT/SBT protocol among certain population subgroups despite current high practice adherence and high levels of perceived acceptability, including ease of use, usefulness and confidence. It is not clear what impact these unresolved questions or concerns may have on practice normalization and multi-year practice sustainment systemwide, including whether targeted late post-implementation strategies are needed to mitigate concerns and promote sustainment when implementation support is withdrawn.
Keywords: Acceptability; Normalization MeAsure Development (NoMAD) survey; Normalization process theory; Practice normalization; Practice sustainment; Spontaneous awakening trial; Spontaneous breathing trial.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Intermountain Health Institutional Review Board reviewed this study and granted approval with a waiver of documentation of informed consent (#1052246). Consent for publication: Not applicable. Competing interests: AJK, JK, DL, AK, DW, CW, CS, CJ, LC, JRJ, LL and CG – the authors have no competing financial or non-financial interests. IP—Dr. Peltan reports funding to his institution from Bluejay Diagnostics and Novartis, both unaffiliated with this research. RH – Dr. Holubkov reports a consulting arrangement with Pfizer Inc (DSMB memberships) unaffiliated with this research. RS—Dr. Srivastava is a physician founder of the I-PASS Patient Safety Institute. His employer, Intermountain Health, owns his equity in the I-PASS Patient Safety Institute. Dr. Srivastava is supported in part by grants from the NIH, CDC, AHRQ and PCORI. Dr. Srivastava has received monetary awards, honorariums, and travel reimbursement from multiple academic and professional organizations for talks about pediatric hospitalist research networks and quality of care.
Figures

References
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38(10):1947–53. - PubMed
-
- Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation. Crit Care Med. 1999;27(12):2609–15. - PubMed
-
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342(20):1471–7. - PubMed
-
- Ely EW, Baker AM, Dunagan DP, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med. 1996;335(25):1864–9. - PubMed
-
- MacIntyre NR, Cook DJ, Ely EW Jr, et al. Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest. 2001;120(6 Suppl):375s–95s. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
