

Ivosidenib for IDH1-Mutant Intrahepatic Cholangiocarcinoma: Insights From a Multicenter Real-World Study
- PMID: 40856270
- PMCID: PMC12379572
- DOI: 10.1111/liv.70295
Ivosidenib for IDH1-Mutant Intrahepatic Cholangiocarcinoma: Insights From a Multicenter Real-World Study
Abstract
Background & aims: Cholangiocarcinoma (CCA) is a rare cancer with limited therapeutic options and a poor prognosis. While first-line combination therapies have improved outcomes, second-line treatment remains challenging. Ivosidenib, an IDH1 inhibitor, has shown promise in treating IDH1 mutant CCA, but real-world data is limited. This study aims to evaluate ivosidenib's efficacy and safety in a large cohort of patients and compare it with second-line chemotherapy.
Methods: This observational, retrospective, multicenter study included patients with advanced IDH1 mutant CCA treated with ivosidenib at 11 European institutions from May 2021 to September 2024. The primary endpoint was progression-free survival (PFS); the main secondary objectives were overall survival (OS), disease control rate (DCR), overall response rate (ORR) and safety. As a pre-planned exploratory objective, mPFS and OS of second-line ivosidenib and FOLFOX/CAPOX were compared by means of inverse probability of treatment weights (IPTW)-adjusted analysis.
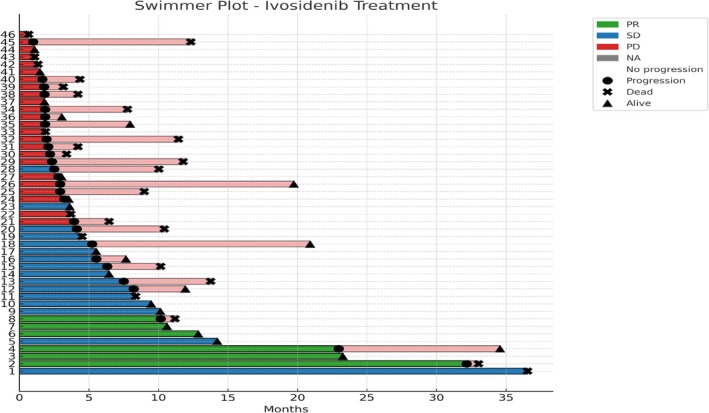
Results: The study included 46 patients treated with Ivosidenib; 43.5% received ivosidenib as second line and 56.5% as ≥ third line. Median PFS and OS were 3.7 (95% CI, 2.2-36.5) and 11.5 months (95% CI, 9.5-36.5). DCR was 50.0%. Grade ≥ 3 adverse events occurred in 8.7% of patients. IPTW-adjusted mPFS was 6.9 months with ivosidenib and 2.1 months with FOLFOX/CAPOX (HR: 0.36, 95% CI, 0.20-0.64, p = 0.0005), while the mOS was 15.9 and 9.0 months with ivosidenib and FOLFOX/CAPOX, respectively (HR: 0.47, 95% CI, 0.23-0.96, p = 0.0405).
Conclusion: This study suggests that ivosidenib is a valid option for patients affected by metastatic IDH1 mutant CCA after at least one line of standard treatment.
© 2025 The Author(s). Liver International published by John Wiley & Sons Ltd.
Conflict of interest statement
M.N. reported receiving travel expenses from AstraZeneca, speaker honoraria from Accademia della Medicina, Incyte and Servier; honoraria from Sandoz, Medpoint SRL, Incyte, AstraZeneca and Servier for editorial collaboration. Consultant honoraria from EMD Serono, Basilea Pharmaceutica, Incyte, MSD Italia, Servier, AstraZeneca and Taiho. L.R. reported receiving consulting fees from AbbVie, AstraZeneca, Basilea, Bayer, BMS, Eisai, Elevar Therapeutics, Exelixis, Genenta, Hengrui, Incyte, Ipsen, IQVIA, Jazz Pharmaceuticals, MSD, Nerviano Medical Sciences, Roche, Servier, Taiho Oncology, Zymeworks; lecture fees from AstraZeneca, Bayer, BMS, Guerbet, Incyte, Ipsen, Roche, Servier; travel expenses from AstraZeneca and Servier; institutional research funding from AbbVie, Agios, AstraZeneca, BeiGene, Eisai, Exelixis, Fibrogen, Incyte, Ipsen, Jazz Pharmaceuticals, Lilly, MSD, Nerviano Medical Sciences, Roche, Servier, Taiho Oncology, TransThera Sciences, Zymeworks. S.L. reported receiving personal honoraria as an invited speaker from Amgen, Astra Zeneca, Bristol‐Myers Squibb, Incyte, GSK, Lilly, Merck Serono, MSD, Pierre‐Fabre, Roche and Servier; participation in an advisory board for Amgen, Astellas, Astra Zeneca, Bayer, Bristol‐Myers Squibb, Daiichi‐Sankyo, GSK, Incyte, Lilly, Merck Serono, MSD, Servier, Takeda, Rottapharm, Beigene, Fosun Pharma and Nimbus Therapeutics. F.P. reported receiving research funding (to Institution) from Lilly, BMS, Incyte, AstraZeneca, Amgen, Agenus, Rottapharm; personal honoraria as an invited speaker from BeiGene, Daiichi‐Sankyo, Seagen, Astellas, Ipsen, AstraZeneca, Servier, Bayer, Takeda, Johnson & Johnson, BMS, MSD, Amgen, Merck‐Serono, Pierre‐Fabre. Advisory/consultancy from BMS, MSD, Amgen, Pierre‐Fabre, Johnson & Johnson, Servier, Bayer, Takeda, Astellas, GSK, Daiichi‐Sankyo, Pfizer, BeiGene, Jazz Pharmaceuticals, Incyte, Rottapharm, Merck‐Serono, Italfarmaco, Gilead, AstraZeneca, Agenus. L.P. reported receiving Advisory/Consultancy from Servier, Astellas, Jazz Pharmaceuticals, AstraZeneca. THE reported receiving Advisory/Consultancy from: MSD, Roche, Sanofi, BMS, AstraZeneca, MSD, Pierre Fabre, Servier, Lilly, Ipsen, Daiichi Sankyo, Takeda. The other authors declare no conflicts of interest.
Figures



References
-
- Izquierdo‐Sanchez L., Lamarca A., La Casta A., et al., “Cholangiocarcinoma Landscape in Europe: Diagnostic, Prognostic and Therapeutic Insights From the ENSCCA Registry,” Journal of Hepatology 76, no. 5 (2022): 1109–1121. - PubMed
-
- Lamarca A., Hubner R. A., David Ryder W., and Valle J. W., “Second‐Line Chemotherapy in Advanced Biliary Cancer: A Systematic Review,” Annals of Oncology 25, no. 12 (2014): 2328–2338. - PubMed
-
- Kelley R. K., Ueno M., Yoo C., et al., “Pembrolizumab in Combination With Gemcitabine and Cisplatin Compared With Gemcitabine and Cisplatin Alone for Patients With Advanced Biliary Tract Cancer (KEYNOTE‐966): A Randomised, Double‐Blind, Placebo‐Controlled, Phase 3 Trial,” Lancet 401, no. 10391 (2023): 1853–1865. - PubMed
-
- Oh D. Y., He A. R., Bouattour M., et al., “Durvalumab or Placebo Plus Gemcitabine and Cisplatin in Participants With Advanced Biliary Tract Cancer (TOPAZ‐1): Updated Overall Survival From a Randomised Phase 3 Study,” Lancet Gastroenterology & Hepatology 9, no. 8 (2024): 694–704. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
