

The association between arrival potassium and 30-day survival following resuscitation from out-of-hospital cardiac arrest: a retrospective cohort study
- PMID: 40859315
- PMCID: PMC12379433
- DOI: 10.1186/s13049-025-01454-8
The association between arrival potassium and 30-day survival following resuscitation from out-of-hospital cardiac arrest: a retrospective cohort study
Abstract
Background: It is unknown whether there is an association between initial serum potassium level and short-term survival in out-of-hospital cardiac arrest (OHCA) survivors. The aim of this study was to describe potential associations between first recorded potassium level and 30-day survival in patients surviving OHCA.
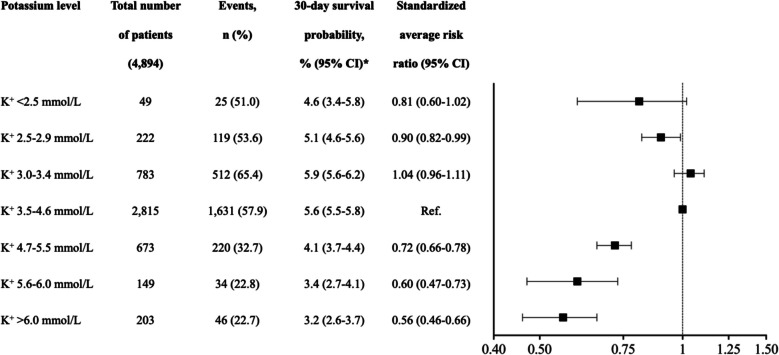
Methods: We identified 4,894 patients who had return of spontaneous circulation (ROSC) at hospital arrival, and a registered post-OHCA serum-potassium value, using Danish nationwide registry data from 2001-2019. Potassium values were divided into seven predefined levels: < 2.5, 2.5-2.9, 3.0-3.4, 3.5-4.6, 4.7-5.5, 5.5-6.0, > 6.0 mmol/L. Thirty-day survival was estimated using a multivariable Cox regression (reference normokalemia 3.5-4.6 mmol/L). The multivariable model included age, sex, Charlson comorbidity index (including chronic kidney disease), witnessed status, performance of bystander cardiopulmonary resuscitation (CPR) and first registered heart rhythm.
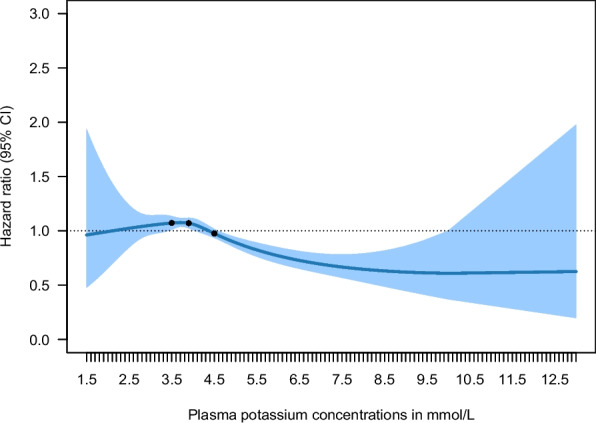
Results: Over the 30-day follow-up period, survival rates in the seven strata were as follows: 25 (51.0%), 119 (53.6%), 512 (65.4%), 1,631 (57.9%), 220 (32.7%), 34 (22.8%), and 46 (22.7%), respectively. Thirty-day survival was significantly lower for all groups with hyperkalemia compared with normokalemia: 4.7-5.5 mmol/L: (average risk ratio (RR): 0.72, 95% confidence interval (95% CI): 0.66-0.78); 5.5-6.0 mmol/L: (average RR: 0.60, 95% CI: 0.47-0.73); > 6.0 mmol/L: (average RR: 0.56, 95% CI: 0.46-0.66). Survival did not differ significantly in patients with hypokalemia compared with normokalemia.
Conclusions: In OHCA survivors, hyperkalemia was associated with reduced 30-day survival compared with normokalemia, independent of age, sex, comorbidity burden and pre-hospital OHCA-characteristics. Conversely, hypokalemia was not associated with reduced 30-day survival.
Keywords: Out-of-hospital cardiac arrest survivors; Potassium; Survival.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Danish Data Protection Agency. Registry-based studies does not require ethical approval by The Danish National Committee on Health Research Ethics. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Kiguchi T, Okubo M, Nishiyama C, Maconochie I, Ong MEH, Kern KB, et al. Out-of-hospital cardiac arrest across the World: first report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2020;152:39–49. 10.1016/j.resuscitation.2020.02.044. - PubMed
-
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197–206. 10.1056/NEJMoa1310519. - PubMed
-
- Sondergaard KB, Riddersholm S, Wissenberg M, Moller Hansen S, Barcella CA, Karlsson L, et al. Out-of-hospital cardiac arrest: 30-day survival and 1-year risk of anoxic brain damage or nursing home admission according to consciousness status at hospital arrival. Resuscitation. 2020;148:251–8. 10.1016/j.resuscitation.2019.12.006. - PubMed
-
- Berg KM, Cheng A, Panchal AR, Topjian AA, Aziz K, Bhanji F, et al. Part 7: systems of care: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S580-604. 10.1161/CIR.0000000000000899. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
