

Blood immunomap for prediction of responses to anti-PD-1 immunotherapy in metastatic non-small cell lung cancer
- PMID: 40860257
- PMCID: PMC12375241
- DOI: 10.1016/j.isci.2025.112804
Blood immunomap for prediction of responses to anti-PD-1 immunotherapy in metastatic non-small cell lung cancer
Abstract
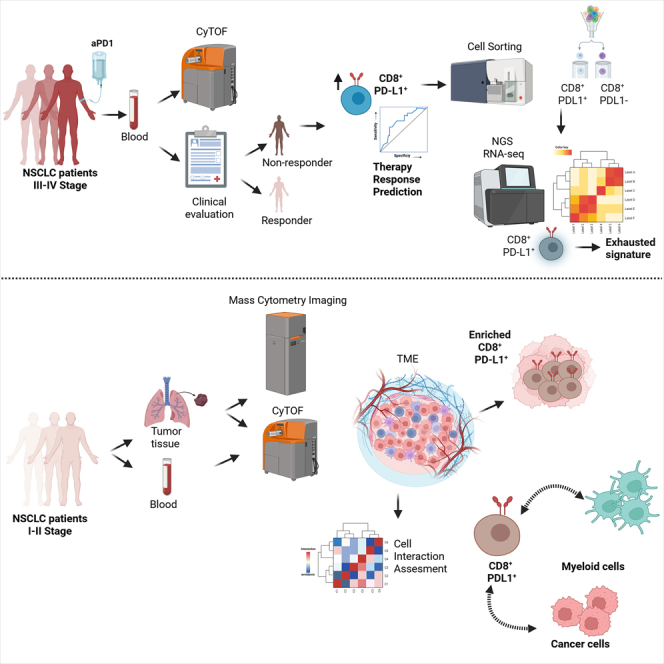
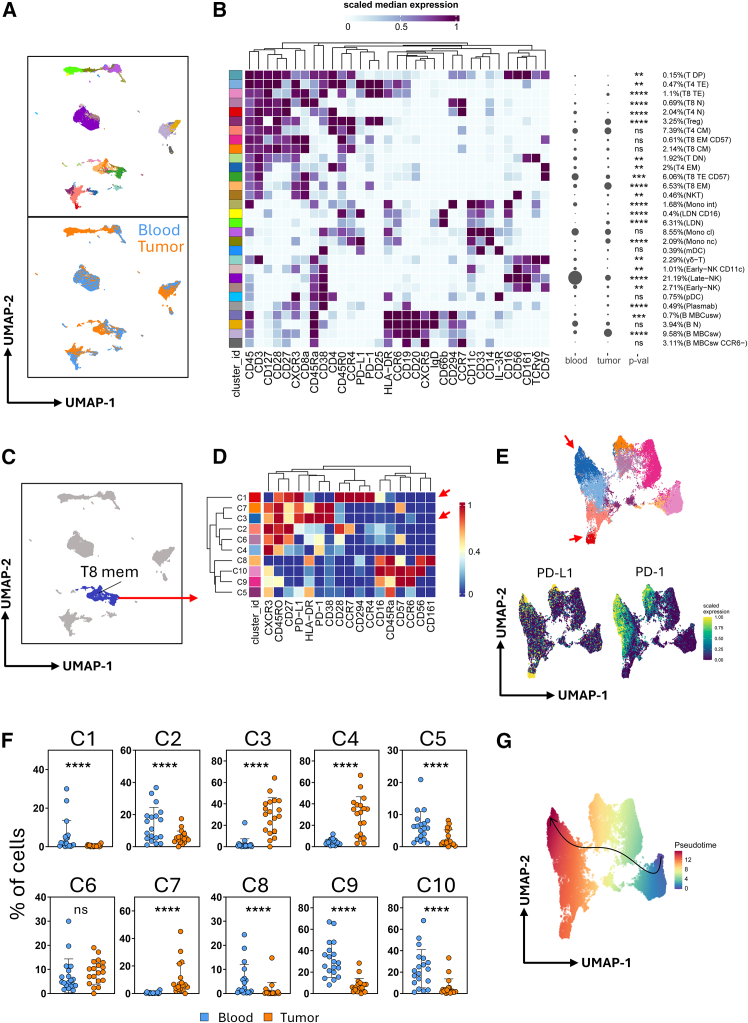
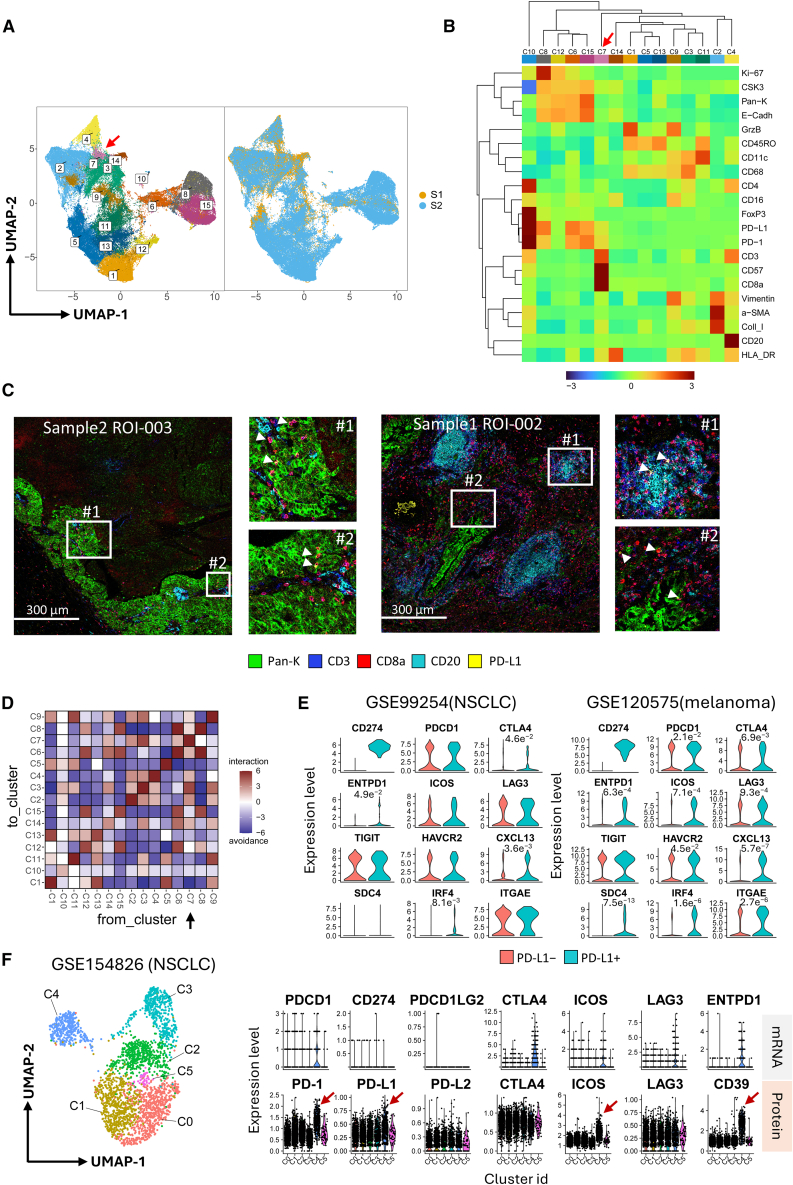
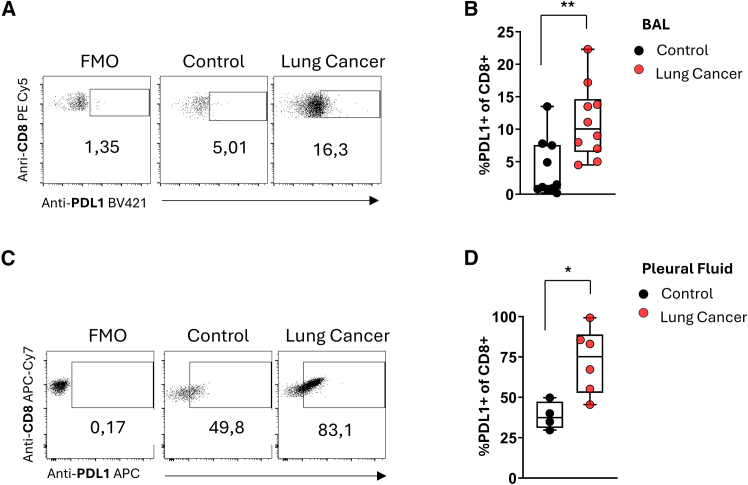
The identification of circulating predictors of response to ICB therapy is vital as very few of them meet the demands of the clinic. Herein, by using high-dimensionality mass cytometry, we designed a blood immunomap in metastatic NSCLC individuals who underwent anti-PD-1 treatment. We identified heightened frequencies of CD8+PD-L1+ T cells in non-responders compared to responders. Notably, imaging mass cytometry data revealed that CD8+PD-L1+ T cells were enriched in tumor biopsies, pleural infusions, and BAL of early-stage NSCLC individuals, proposing this cells subset as candidate not only for the advanced but also for early disease detection. Transcriptomic analysis unveiled that CD8+PD-L1+ T cells displayed an exhausted phenotype related to their increased frequencies to non-responders to immunotherapy, and gene signatures correlated with the overall survival of an independent cohort. Overall, our study pinpoints immune-related events which may benefit the quest for detection of predictive biomarkers of immunotherapy responses.
Keywords: Cancer; Transcriptomics.
© 2025 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Garon E.B., Hellmann M.D., Rizvi N.A., Carcereny E., Leighl N.B., Ahn M.J., Eder J.P., Balmanoukian A.S., Aggarwal C., Horn L., et al. Five-Year Overall Survival for Patients With Advanced Non‒Small-Cell Lung Cancer Treated With Pembrolizumab: Results From the Phase I KEYNOTE-001 Study. J. Clin. Oncol. 2019;37:2518–2527. doi: 10.1200/JCO.19.00934. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
