

Evaluation of Tideglusib as a Disease Modifying Therapy in Murine Models of Arrhythmogenic Cardiomyopathy
- PMID: 40866040
- PMCID: PMC12399120
- DOI: 10.1016/j.jacbts.2025.03.013
Evaluation of Tideglusib as a Disease Modifying Therapy in Murine Models of Arrhythmogenic Cardiomyopathy
Abstract
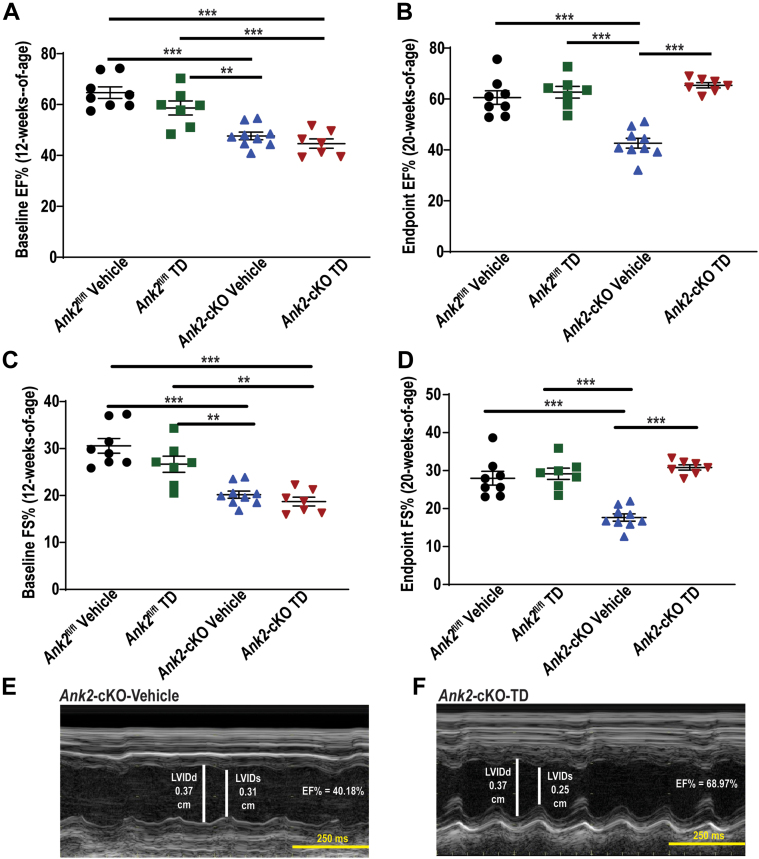
Arrhythmogenic cardiomyopathy (ACM) is an inherited heart disease, and current pharmacological therapies are directed toward the management of electrical manifestations. To date, none address the underlying pathophysiology of this progressive condition. We evaluated the therapeutic efficacy of Tideglusib (TD) in Ank2 cardio-selective-knockout and homozygous desmoglein-2 mutant ACM mouse models. TD was able to prevent and reverse the reduced cardiac function in treated mice. Moreover, TD-treated adult mice displayed a reduction in ventricular arrhythmia following adrenergic stimulation. We provide compelling preclinical data for TD as a potential therapy for patients with ACM.
Keywords: GSK-3β; Tideglusib; ankyrin-B; arrhythmia; arrhythmogenic cardiomyopathy; cardiovascular disease; desmoglein-2.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The authors are supported by National Institutes of Health grants HL146969 and HL175380 to Dr Refaey; HL135754 to Dr Mohler; HL171689, HL156652, and HL165751 to Dr Hund; a grant from the Ohio State Frick Center for Heart Failure and Arrhythmia, the Leducq Foundation (TNE FANTASY 19CV03) to Dr Mohler; and the JB Cardiovascular Fellowship. Dr Roberts has been named as an inventor on a patent application that has been filed for use of Tideglusib as a therapeutic for ACM. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures









References
-
- Frank R., Fontaine G., Vedel J., et al. [Electrocardiology of 4 cases of right ventricular dysplasia inducing arrhythmia] Archives des maladies du coeur et des vaisseaux. 1978;71:963–972. - PubMed
-
- Dungan W.T., Garson A., Jr., Gillette P.C. Arrhythmogenic right ventricular dysplasia: a cause of ventricular tachycardia in children with apparently normal hearts. Am Heart J. 1981;102:745–750. - PubMed
-
- Corrado D., Perazzolo Marra M., Zorzi A., et al. Diagnosis of arrhythmogenic cardiomyopathy: the Padua criteria. Int J Cardiol. 2020;319:106–114. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
