

Adjuvant icotinib for resected EGFR-mutated stage II-IIIA non-small-cell lung cancer (ICTAN, GASTO1002): a randomized comparison study
- PMID: 40866342
- PMCID: PMC12391381
- DOI: 10.1038/s41392-025-02358-w
Adjuvant icotinib for resected EGFR-mutated stage II-IIIA non-small-cell lung cancer (ICTAN, GASTO1002): a randomized comparison study
Abstract
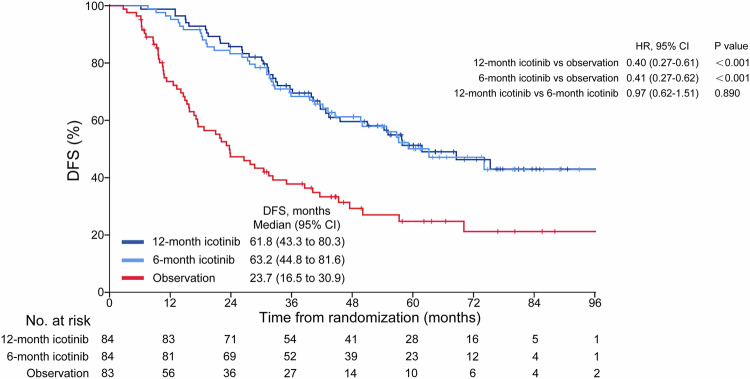
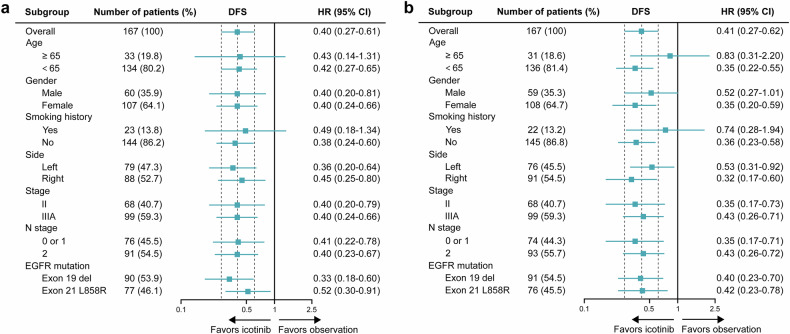
The efficacy, safety and ideal treatment duration of an adjuvant epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) for patients with resected EGFR-mutated non-small-cell lung cancer (NSCLC) were not known until 2014, when this study was initiated. In this phase 3 ICTAN trial (GASTO1002, NCT01996098), patients with completely resected, EGFR-mutated, stage II-IIIA NSCLC after adjuvant chemotherapy were assigned in a 1:1:1 ratio to receive icotinib (125 mg, three times daily) for 12 months, to receive icotinib for 6 months, or to undergo observation. The primary endpoint was disease-free survival (DFS). This trial was terminated early. A total of 251 patients were randomized. Adjuvant icotinib for 12 months significantly improved DFS (hazard ratio [HR]: 0.40, 95% confidence interval [CI], 0.27-0.61; P < 0.001) and overall survival (OS; HR: 0.55, 95% CI, 0.32-0.96; P = 0.032) compared with observation. Adjuvant icotinib of 6 months also significantly improved DFS (HR: 0.41, 95% CI, 0.27-0.62; P < 0.001) and OS (HR: 0.56, 95% CI, 0.32-0.98; P = 0.038) compared with observation. Adjuvant icotinib for 12 months did not improve DFS (HR: 0.97; P = 0.89) or OS (HR: 1.00; P = 0.99) compared with 6 months of this drug. Rates of adverse events of grade 3 or higher were 8.3%, 6.0% and 2.4% for the 12-month icotinib, 6-month icotinib, and observation groups, respectively. Adjuvant icotinib for 12 months or 6 months following adjuvant chemotherapy improved DFS and OS compared with observation in patients with resected EGFR-mutated stage II-IIIA NSCLC with a manageable safety profile, supporting it as a potential treatment option.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: All authors declare no competing interests.
Figures


References
-
- Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.74, 229–263 (2024). - PubMed
-
- Thai, A. A., Solomon, B. J., Sequist, L. V., Gainor, J. F. & Heist, R. S. Lung cancer. Lancet398, 535–554 (2021). - PubMed
-
- Datta, D. & Lahiri, B. Preoperative evaluation of patients undergoing lung resection surgery. Chest123, 2096–2103 (2003). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
