

Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of frontotemporal dementia
- PMID: 40866991
- PMCID: PMC12392567
- DOI: 10.1186/s13024-025-00882-5
Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of frontotemporal dementia
Abstract
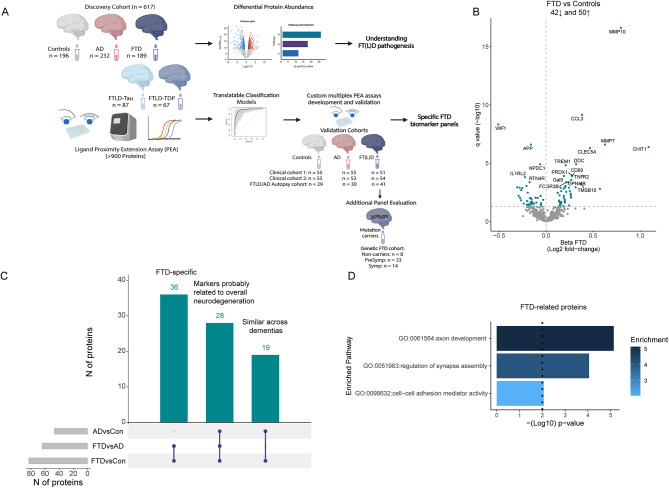
Background: Diagnosis of Frontotemporal dementia (FTD) and its specific underlying neuropathologies (frontotemporal lobar degeneration; FTLD-Tau and FTLD-TDP) are challenging, and thus, fluid biomarkers are needed to improve diagnostic accuracy.
Methods: We used proximity extension assays to analyze 665 proteins in cerebrospinal fluid (CSF) samples from a multicenter cohort, which included patients with FTD (n = 189), Alzheimer’s Disease dementia (AD; n = 232), and cognitively unimpaired individuals (n = 196). In a subset, FTLD neuropathology was determined based on phenotype or genotype (FTLD-Tau = 87 and FTLD-TDP = 67). Differences in protein expression profiles were analyzed using nested linear models. Penalized generalized linear modeling was used to identify classification protein panels, which were translated to custom multiplex assays and validated in two clinical cohorts (cohort 1: n = 161; cohort 2: n = 162), one autopsy-confirmed cohort (n = 100), and one genetic cohort (n = 55).
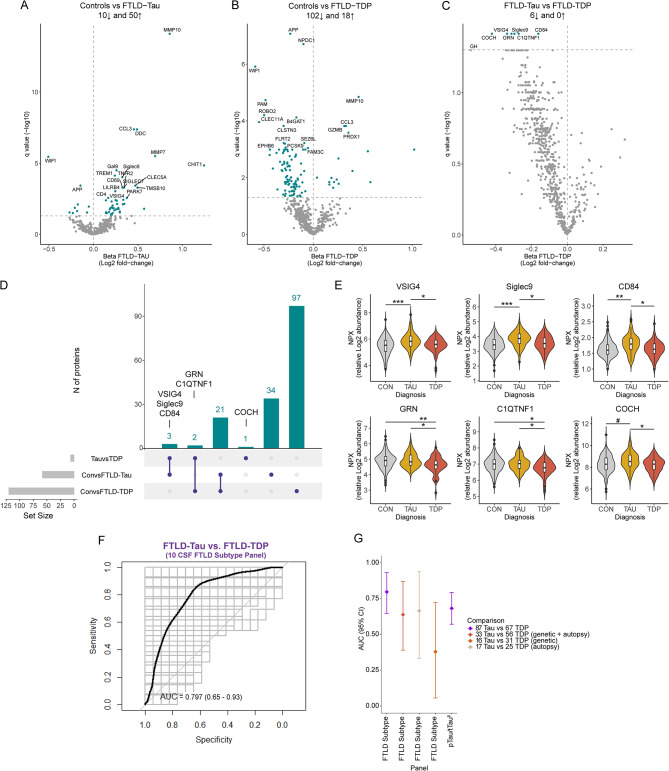
Results: Forty-three proteins were differentially regulated in FTD compared to controls and AD, reflecting axon development, regulation of synapse assembly, and cell-cell adhesion mediator activity pathways. Classification analysis identified a 14- and 13-CSF protein panel that discriminated FTD from controls (FTD diagnostic panel, AUC: 0.96) or AD (FTD differential diagnostic panel, AUC: 0.91). Custom multiplex panels confirmed the strong discriminative performancen between FTD and controls (AUCs > 0.96) and between FTD and AD (AUCs > 0.88) across three validation cohorts, including one with autopsy confirmation (AUCs > 0.90). Validation in genetic FTD (including C9orf72, GRN, and MAPT mutation carriers) revealed high accuracy of the FTD diagnostic panel in identifying both the presymptomatic (AUCs > 0.95) and symptomatic (AUC: 1) stages. Six proteins were differentially regulated between FTLD-TDP and FTLD-Tau. However, a reproducible classification model could not be generated (AUC: 0.80).
Conclusions: Overall, this study introduces novel FTD-specific biomarker panels with potential use in diagnostic settings.
Supplementary Information: The online version contains supplementary material available at 10.1186/s13024-025-00882-5.
Keywords: Biomarkers; CSF; FTD; FTLD; Proteomics; TDP43; Tau.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approval was given by the institutional ethical review boards of each center. Written informed consent was obtained from all participants or their authorized representatives. Consent for publication: Not applicable. Competing interests: Y.H., C.P., E.E., S.B., L.M, J.S., J.H., H.R., W.H., A.S., A.C.-P, and D.I. declare no competing interest. M.C. has been an invited speaker at Eisai, is an associate editor at Alzheimer´s Research & Therapy and has been an invited writer for Springer Healthcare. L.V. received a grant for CORAL consortium by Olink proteomics. D.I. is a Scientific Advisory Board Member for Denali Therapeutics. D.A. participated in advisory boards from Fujirebio-Europe and Roche Diagnostics and received speaker honoraria from Fujirebio-Europe, Roche Diagnostics, Nutricia, Krka Farmacéutica S.L., Zambon S.A.U. and Esteve Pharmaceuticals. S.A. D.A., and A.L. declare a filed patent application (Title: Markers of synaptopathy in neurodegenerative disease; Applicant: Fundació Institut de Recerca de l’Hospital de la Santa Creu i Sant Pau, Inventors: Olivia BELBIN; Alberto LLEÓ; Alejandro BAYÉS; Juan FORTEA; Daniel ALCOLEA; Application number: PCT/EP2019/056535; International Publication Number: WO 2019/175379 A1; Current status: Active. Licensed to ADx Neurociences NV (Ghent, Belgium); this patent is not related to any specific aspect of the current manuscript). S.E. received personal fees from Eisai (paid to institution), personal fees from icometrix (paid to institution), personal fees from Novartis (paid to institution), personal fees from Roche (paid to institution) and personal fees from Roche and personal fees from Biogen, all outside the submitted work. W.F. has performed contract research for Biogen MA Inc, and Boehringer Ingelheim. W.F. has been an invited speaker at Boehringer Ingelheim, Biogen MA Inc, Danone, Eisai, WebMD Neurology (Medscape), Springer Healthcare. W.F. is consultant to Oxford Health Policy Forum CIC, Roche, and Biogen MA Inc. WF participated in advisory boards of Biogen MA Inc and Roche. All funding is paid to her institution. W.F. is a member of the steering committee of PAVE, and Think Brain Health. W.F. was associate editor of Alzheimer’s Research & Therapy in 2020/2021 and is currently an associate editor at Brain. C.E.T. has a collaboration contract with ADx Neurosciences, Quanterix, and Eli Lilly, performed contract research or received grants from AC-Immune, Axon Neurosciences, Bioconnect, Bioorchestra, Brainstorm Therapeutics, Celgene, EIP Pharma, Eisai, Grifols, Novo Nordisk, PeopleBio, Roche, Toyama, and Vivoryon. She serves on editorial boards of Medidact Neurologie/Springer, Alzheimer’s Research & Therapy, Neurology: Neuroimmunology & Neuroinflammation, and is editor of a Neuromethods book Springer. She had speaker contracts for Roche, Grifols, and Novo Nordisk.
Figures



Update of
-
Large-scale CSF proteome profiling identifies biomarkers for accurate diagnosis of Frontotemporal Dementia.medRxiv [Preprint]. 2024 Aug 20:2024.08.19.24312100. doi: 10.1101/2024.08.19.24312100. medRxiv. 2024. Update in: Mol Neurodegener. 2025 Aug 27;20(1):93. doi: 10.1186/s13024-025-00882-5. PMID: 39228745 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
