

Circulating Lipid Profiles Indicate Incomplete Metabolic Recovery After Weight Loss, Suggesting the Need for Additional Interventions in Severe Obesity
- PMID: 40867557
- PMCID: PMC12383904
- DOI: 10.3390/biom15081112
Circulating Lipid Profiles Indicate Incomplete Metabolic Recovery After Weight Loss, Suggesting the Need for Additional Interventions in Severe Obesity
Erratum in
-
Correction: Onoiu et al. Circulating Lipid Profiles Indicate Incomplete Metabolic Recovery After Weight Loss, Suggesting the Need for Additional Interventions in Severe Obesity. Biomolecules 2025, 15, 1112.Biomolecules. 2025 Dec 25;16(1):34. doi: 10.3390/biom16010034. Biomolecules. 2025. PMID: 41594720 Free PMC article.
Abstract
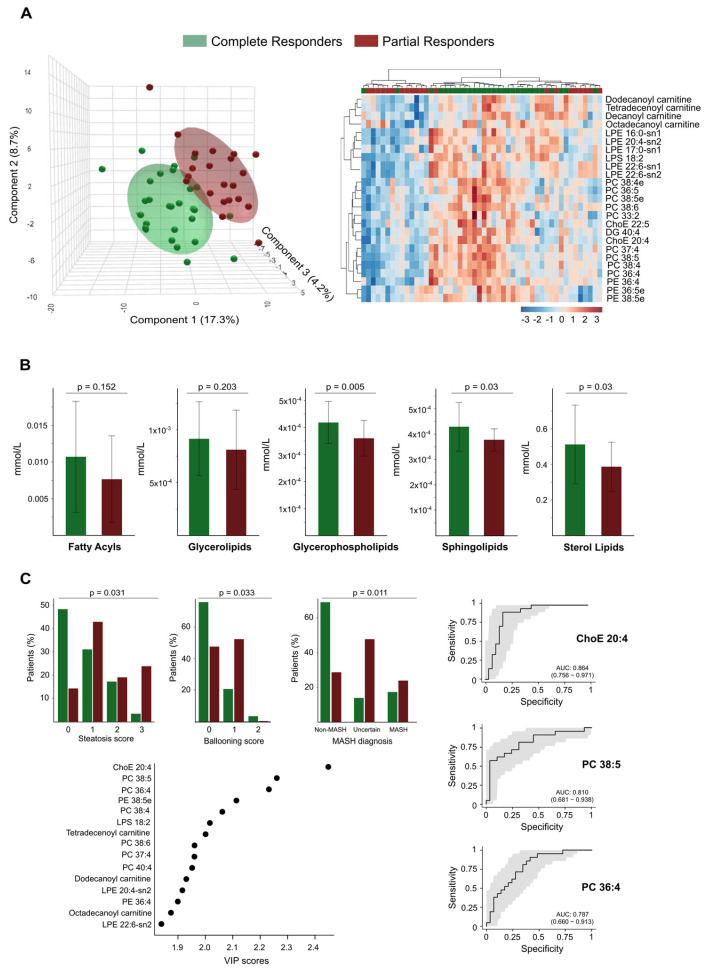
The effects of long-term adjustments in body weight on the lipid balance in patients with severe obesity are not well understood. This study aimed to evaluate a non-invasive lipidomic approach to identifying biomarkers that could help predict which patients may require additional therapies before and after weight loss. Using mass spectrometry, 275 lipid species were analysed in non-obese controls, patients with severe obesity, and patients one year after bariatric surgery. The results showed that severe obesity disrupts lipid pathways, contributing to lipotoxicity, inflammation, mitochondrial stress, and abnormal lipid metabolism. Although weight loss improved these disturbances, surgery did not fully normalise the lipid profiles of all patients. Outcomes varied depending on their baseline liver health and genetic differences. Persistent alterations in cholesterol handling, membrane composition, and mitochondrial function were observed in partial responders. Elevated levels of sterol lipids, glycerophospholipids, and sphingolipids emerged as markers of complete metabolic recovery, identifying candidates for targeted post-surgical interventions. These findings support the use of lipidomics to personalise obesity treatment and follow-up.
Keywords: biomarkers; fatty acid metabolism; lipidomics; metabolic surgery; obesity; oxylipins; precision medicine.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures





References
-
- UN . World Population Prospects 2024. United Nations, Department of Economic and Social Affairs, Population Division; New York, NY, USA: 2024. [(accessed on 17 June 2025)]. Online Edition. Available online: https://population.un.org/wpp/
-
- Rubino F., Cummings D.E., Eckel R.H., Cohen R.V., Wilding J.P.H., Brown W.A., Stanford F.C., Batterham R.L., Farooqi I.S., Farpour-Lambert N.J., et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13:221–262. doi: 10.1016/S2213-8587(24)00316-4. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
