

Comparative Safety of Anticoagulant, Antiplatelet and the Combination of Both for Acute Coronary Syndrome: A Systematic Review and Network Meta-Analysis
- PMID: 40868278
- PMCID: PMC12383640
- DOI: 10.3390/biomedicines13082027
Comparative Safety of Anticoagulant, Antiplatelet and the Combination of Both for Acute Coronary Syndrome: A Systematic Review and Network Meta-Analysis
Abstract
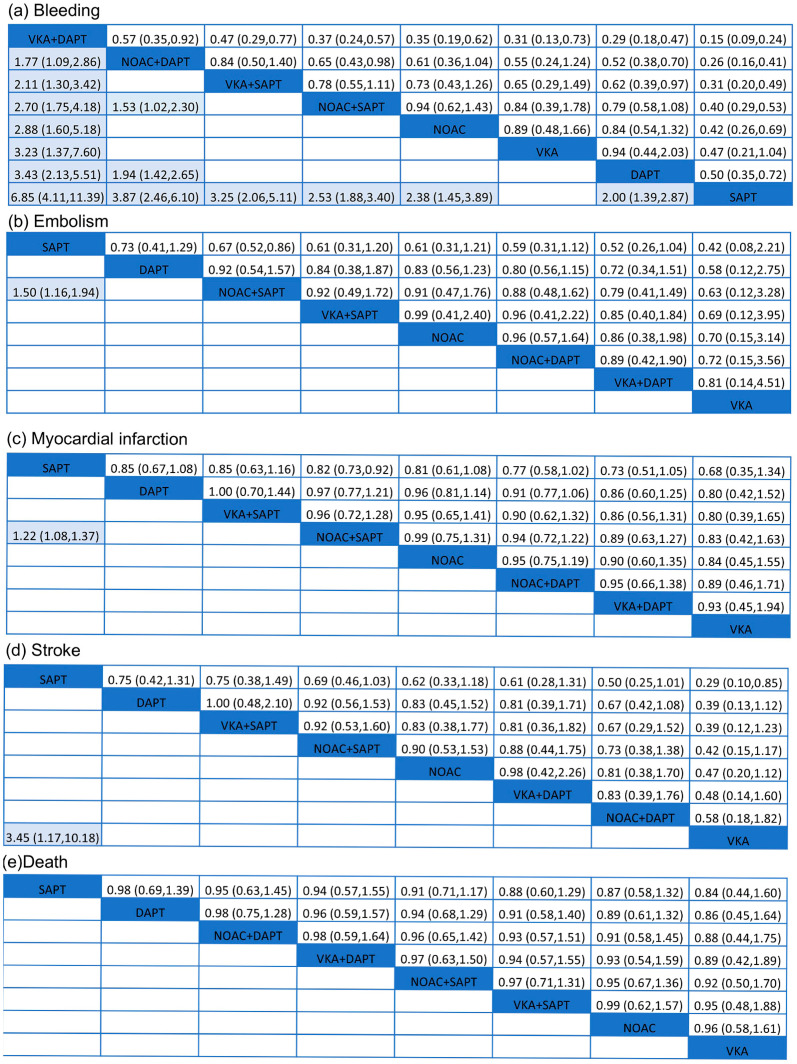
Background: Antithrombotic therapy plays an important role in acute coronary syndrome (ACS). The combination of anticoagulant and antiplatelet therapy resulted in fewer complications and stronger potency compared to traditional monotherapy. Our net meta-analysis aimed to compare and rank the safety of different treatments used in patients with ACS. Method: We conducted a search for trials in three prominent databases. The main objective of our investigation was to assess hemorrhage. Additional outcomes included mortality, myocardial infarction, stroke, and embolism. We used a frequentist network meta-analysis with a random-effects model to, directly and indirectly, compare safety across different antithrombotic strategies. Result: A total of 30 randomized clinical trials were included in this net meta-analysis with 135,471 ACS patients. In these eight different antithrombotic therapies, SAPT (single-agent platelet inhibitor therapy) showed the lowest risk of bleeding (SUCRA = 0.5%). The highest risk of bleeding was observed in VKA (vitamin K antagonists) + DAPT (dual antiplatelet therapy) (SUCRA = 99.8%). Bleeding among NOAC (non-vitamin K antagonist oral anticoagulants) + DAPT was found to be higher than DAPT (OR = 1.94, 95% CI = 1.42-2.65). NOAC + SAPT significantly reduced the embolism (OR = 1.50, 95% CI = 1.16-1.94) and myocardial infarction (OR = 1.22, 95% CI = 1.08-1.37) events compared with SAPT. In addition, VKA significantly reduced the rate of stroke compared with SAPT (OR = 3.45, 95% CI = 1.17-10.18). However, no significant difference was observed in death events among these eight antithrombotic therapies. Conclusions: We advise against the use of SAPT in ACS due to its elevated risk of embolism, myocardial infarction, and stroke. It is important to mention that the combination of NOAC and SAPT has a lower incidence of myocardial infarction, bleeding and embolism problems. Therefore, the combination of NOAC and SAPT may be the optimal approach to achieve a balance between the risks of bleeding and embolism. This meta-analysis was registered in PROSPERO with the registration number CRD42024542826.
Keywords: acute coronary syndrome; anticoagulant; antiplatelet; network meta-analysis; safety.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., Anderson C.A.M., Arora P., Avery C.L., Baker-Smith C.M., Beaton A.Z., Boehme A.K., Buxton A.E., et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2023;147:E93–E621. doi: 10.1161/CIR.0000000000001123. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
