

Uncommon and Accessory Electrocardiographic Findings in Brugada Syndrome: A Review
- PMID: 40869720
- PMCID: PMC12387241
- DOI: 10.3390/jcm14165895
Uncommon and Accessory Electrocardiographic Findings in Brugada Syndrome: A Review
Abstract
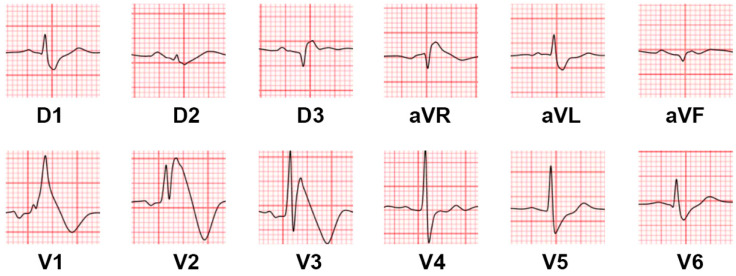
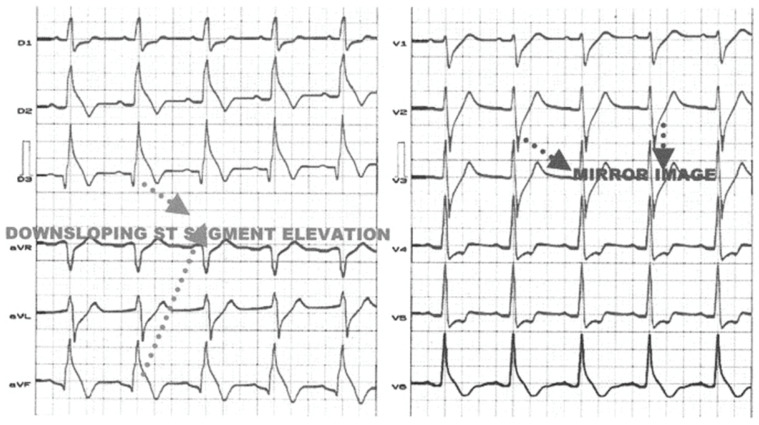
Brugada syndrome (BrS) is a cardiac arrhythmic disorder associated with distinctive electrocardiographic (ECG) abnormalities and an increased risk of sudden cardiac death due to ventricular arrhythmias. While the classic BrS ECG pattern is a coved ST-segment elevation in the right precordial leads, a wide spectrum of atypical ECG presentations can mislead the diagnosis. This review discusses rare and under-recognized ECG findings associated with BrS, including its coexistence with right and left bundle branch block, alterations in peripheral leads and in the morphology of the QRS complex, as well as atrioventricular conduction abnormalities. Emphasis is placed on the clinical relevance of these findings, their underlying electrophysiological mechanisms, and their prognostic implications. Recognizing these atypical manifestations is critical to avoid misdiagnosing or failing to recognize the condition in patients with BrS.
Keywords: Brugada syndrome; electrocardiography; sudden cardiac death; ventricular arrhythmias.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
