

Total Intravenous Versus Inhalational Anesthesia in High-Grade Glioma Surgery: A Systematic Review and Meta-Analysis
- PMID: 40870507
- PMCID: PMC12387908
- DOI: 10.3390/medicina61081463
Total Intravenous Versus Inhalational Anesthesia in High-Grade Glioma Surgery: A Systematic Review and Meta-Analysis
Abstract
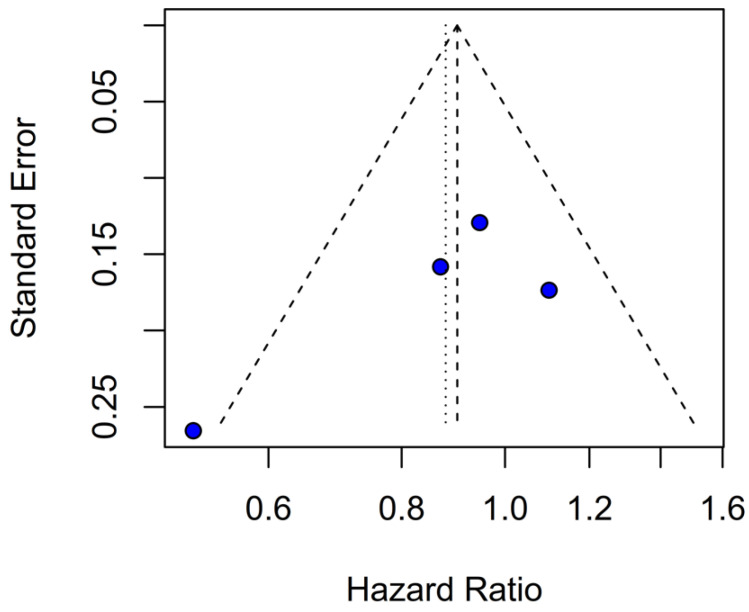
Background and Objectives: High-grade gliomas (HGGs) are aggressive primary brain tumors with a poor prognosis despite multimodal treatment. The anesthetic technique used during surgery may influence tumor progression and survival, but its role in HGGs remains unclear. This meta-analysis evaluated the effect of total intravenous anesthesia (TIVA) versus inhalational anesthesia (INHA) on overall survival (OS) and progression-free survival (PFS) in HGG patients. Materials and Methods: A systematic search was conducted in PubMed, Scopus, and Cochrane databases for studies assessing the impact of TIVA versus INHA on OS and PFS in HGG patients. Statistical analysis was performed using R version 4.3.1. Heterogeneity across studies was quantified using the Cochrane Q test alongside the I2 statistic. A random-effects model was employed to derive the pooled hazard ratios (HRs). Results: A total of five studies involving 827 participants (mean age 58 years, mean females 38%) were included, of whom 406 (49%) received TIVA. No statistically significant differences were observed in OS (HR 0.77; 95% CI [0.58-1.02]; p = 0.07; I2 = 67%) or PFS (HR 0.88; 95% CI [0.70-1.10]; p = 0.27; I2 = 51%) between the groups. A subgroup analysis revealed that TIVA was associated with improved OS in patients with grade IV tumors (HR 0.70; 95% CI [0.51-0.96]; p = 0.03), while no significant effect was observed in the mixed grade III-IV subgroup. However, the test for subgroup differences was not statistically significant (p = 0.0669), and this finding should be interpreted with caution. No significant differences were observed in median OS or PFS, or in single-arm meta-analyses. Conclusions: This meta-analysis found no statistically significant differences in overall or progression-free survival between TIVA and INHA in patients undergoing surgery for HGGs. Although a subgroup analysis suggested a possible survival advantage of TIVA in grade IV tumors, the lack of a statistically significant subgroup difference test limits the strength of this finding. Further investigation is needed to determine whether anesthetic technique influences outcomes in this subgroup.
Keywords: glioblastoma; high-grade gliomas; inhalational anesthesia (INHA); total intravenous anesthesia (TIVA).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



























Similar articles
-
Intravenous versus inhalational maintenance of anaesthesia for postoperative cognitive outcomes in elderly people undergoing non-cardiac surgery.Cochrane Database Syst Rev. 2018 Aug 21;8(8):CD012317. doi: 10.1002/14651858.CD012317.pub2. Cochrane Database Syst Rev. 2018. PMID: 30129968 Free PMC article.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Antiangiogenic therapy for high-grade glioma.Cochrane Database Syst Rev. 2014 Sep 22;(9):CD008218. doi: 10.1002/14651858.CD008218.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2018 Nov 22;11:CD008218. doi: 10.1002/14651858.CD008218.pub4. PMID: 25242542 Updated.
-
Treatment options for progression or recurrence of glioblastoma: a network meta-analysis.Cochrane Database Syst Rev. 2021 May 4;5(1):CD013579. doi: 10.1002/14651858.CD013579.pub2. Cochrane Database Syst Rev. 2021. PMID: 34559423 Free PMC article.
-
Radiotherapy for diffuse brainstem glioma in children and young adults.Cochrane Database Syst Rev. 2016 Jun 27;2016(6):CD010439. doi: 10.1002/14651858.CD010439.pub2. Cochrane Database Syst Rev. 2016. PMID: 27378212 Free PMC article.
References
-
- Dong J., Zeng M., Ji N., Hao S., Zhou Y., Gao Z., Gu H., Zhang L., Ma D., Peng Y., et al. Impact of Anesthesia on Long-term Outcomes in Patients with Supratentorial High-grade Glioma Undergoing Tumor Resection: A Retrospective Cohort Study. J. Neurosurg. Anesthesiol. 2020;32:227–233. doi: 10.1097/ANA.0000000000000588. - DOI - PubMed
-
- Kumaria A., Hughes M., Fenner H., Moppett I.K., Smith S.J. Total intravenous anaesthesia with propofol and remifentanil is associated with reduction in operative time in surgery for glioblastoma when compared with inhalational anaesthesia with sevoflurane. J. Clin. Neurosci. 2024;120:191–195. doi: 10.1016/j.jocn.2024.01.022. - DOI - PubMed
-
- Schmoch T., Jungk C., Bruckner T., Haag S., Zweckberger K., von Deimling A., Brenner T., Unterberg A., Weigand M.A., Uhle F., et al. The anesthetist’s choice of inhalational vs. intravenous anesthetics has no impact on survival of glioblastoma patients. Neurosurg. Rev. 2021;44:2707–2715. doi: 10.1007/s10143-020-01452-7. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
