

Coronary Angioplasty with Drug-Coated Balloons: Pharmacological Foundations, Clinical Efficacy, and Future Directions
- PMID: 40870515
- PMCID: PMC12387977
- DOI: 10.3390/medicina61081470
Coronary Angioplasty with Drug-Coated Balloons: Pharmacological Foundations, Clinical Efficacy, and Future Directions
Abstract
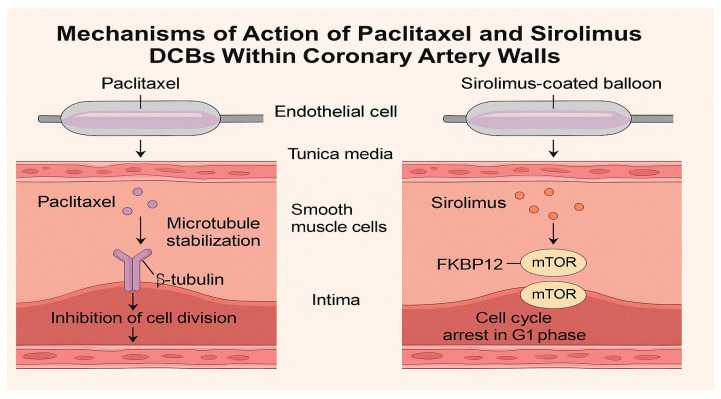
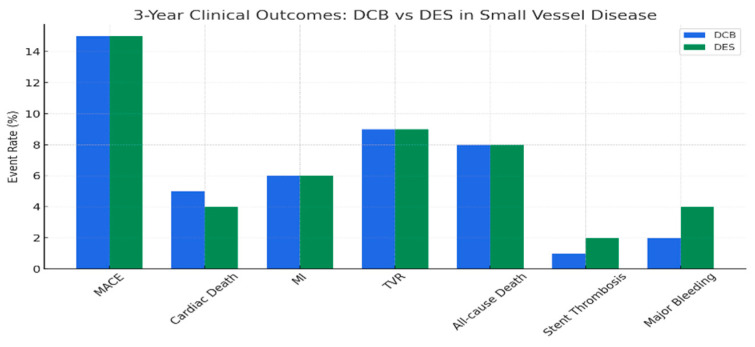
Drug-coated balloons (DCBs) have transformed percutaneous coronary intervention (PCI) by delivering antiproliferative drugs directly to the arterial wall, offering a stent-less approach that mitigates the risks associated with permanent metallic implants. Initially developed for in-stent restenosis (ISR), DCBs have demonstrated robust efficacy in reducing neointimal hyperplasia and target lesion revascularization (TLR) rates across diverse coronary lesions, including small vessel disease (SVD), de novo lesions, and complex anatomies such as bifurcation lesions. Paclitaxel-coated balloons have long been the cornerstone of DCB therapy due to their established clinical outcomes, but sirolimus-coated balloons are emerging as a promising alternative with potentially superior safety profiles and sustained drug release. The pharmacological mechanism of DCBs relies on rapid drug transfer during brief balloon inflation, achieving high local concentrations without residual foreign material. Landmark trials, such as BASKET-SMALL 2, RESTORE SVD, and AGENT IDE, have demonstrated comparable or non-inferior outcomes of DCBs versus drug-eluting stents (DESs) in specific settings, with lower rates of stent thrombosis and shorter dual antiplatelet therapy (DAPT) requirements. Despite these advances, challenges persist, including optimizing drug formulations, ensuring uniform delivery, and addressing calcified lesions. Ongoing research into novel coatings, dual-drug systems, and artificial intelligence (AI)-guided interventions is poised to redefine PCI strategies. This review provides a comprehensive analysis of drug-coated balloon (DCB) angioplasty, not limited to specific clinical scenarios such as in-stent restenosis, small vessel disease, or bifurcation lesions, highlighting their transformative role in coronary artery disease (CAD) management. Instead, it addresses the full spectrum of pharmacological principles, mechanisms of action, clinical indications, comparative efficacy across various coronary artery disease contexts, and future directions of DCBs.
Keywords: de novo lesions; drug-coated balloons; in-stent restenosis; paclitaxel; percutaneous coronary intervention; sirolimus; small vessel disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Jeremias A., Davies J.E., Maehara A., Matsumura M., Schneider J., Tang K., Talwar S., Marques K., Shammas N.W., Gruberg L., et al. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovasc. Interv. 2019;12:1991–2001. doi: 10.1016/j.jcin.2019.05.054. - DOI - PubMed
-
- Serruys P.W., Luijten H.E., Beatt K.J., Geuskens R., de Feyter P.J., van den Brand M., Reiber J.H., ten Katen H.J., van Es G.A., Hugenholtz P.G. Incidence of restenosis after successful coronary angioplasty: A time-related phenomenon. A quantitative angiographic study in 342 consecutive patients at 1, 2, 3, and 4 months. Circulation. 1988;77:361–371. doi: 10.1161/01.CIR.77.2.361. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
