

A Novel Approach to Estimate the Impact of PCV20 Immunization in Children by Incorporating Indirect Effects to Generate the Number Needed to Vaccinate
- PMID: 40872892
- PMCID: PMC12389863
- DOI: 10.3390/vaccines13080805
A Novel Approach to Estimate the Impact of PCV20 Immunization in Children by Incorporating Indirect Effects to Generate the Number Needed to Vaccinate
Abstract
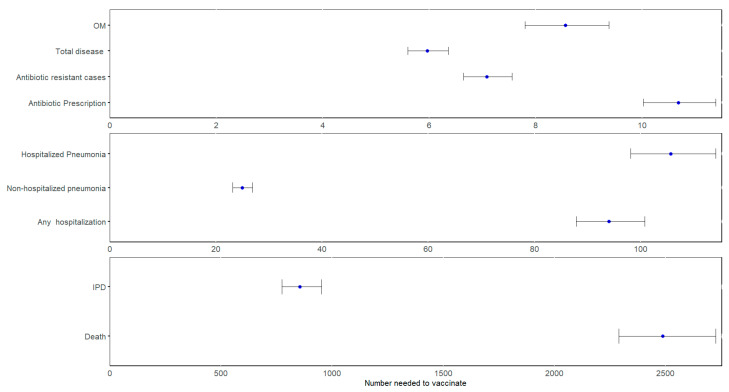
Background/Objectives: The number needed to vaccinate (NNV) is a metric commonly used to evaluate the public health impact of a vaccine as it represents the number of individuals that must be vaccinated to prevent one case of disease. Traditional calculations may underestimate vaccine benefits by neglecting indirect effects and duration of protection (DOP), resulting in NNV overestimation. This study evaluated the NNV for the pediatric 20-valent pneumococcal conjugate (PCV20) US immunization program, as compared to PCV13, with a unique approach to NNV. Methods: A multi-cohort, population-based Markov model accounting for indirect effects was employed to calculate the NNV of PCV20 to avert a case of pneumococcal disease, invasive pneumococcal disease (IPD), hospitalized non-bacteremic pneumonia (NBP), ambulatory NBP, and otitis media (OM), as well as to prevent antibiotic-resistant cases and antibiotic prescriptions. Results: The mean NNV over a 25-year time horizon to prevent one case of pneumococcal disease was 6, with NNVs of 854 for IPD, 106 for hospitalized NBP, 25 for outpatient NBP, and 9 for OM, 11 for a course of antibiotic, and 4 for resistant disease. The mean NNV per year decreased over time, reflecting the DOP and increasing indirect effects over time. Conclusions: This study presents a novel approach to NNVs and shows that relatively few vaccinations are required to prevent disease. The decrease in NNV over time highlights the necessity of including DOP and indirect effects in NNV calculations, ensuring a more realistic assessment of a vaccine's impact.
Keywords: PCVs; full value of vaccine assessment; number needed to vaccinate; pneumococcal; vaccination.
Conflict of interest statement
Ruth Chapman, Desmond Dillon-Murphy are employees of PPD™ Evidera™, which received funding from Pfizer in connection with the development of this manuscript and study. Mark H. Rozenbaum, Maria J. Tort, Blair Capitano, Benjamin M. Althouse, Alejandro Cane are employees and shareholders of Pfizer.
Figures


Similar articles
-
Pneumococcal vaccination for new residents entering older adult care homes in England: national observational surveillance study.Lancet Healthy Longev. 2025 Jun;6(6):100726. doi: 10.1016/j.lanhl.2025.100726. Epub 2025 Jul 1. Lancet Healthy Longev. 2025. PMID: 40614750
-
Cost-effectiveness analysis of the pediatric 20-valent pneumococcal conjugate vaccine compared with lower-valent alternatives in Argentina.Vaccine. 2024 Oct 3;42(23):126043. doi: 10.1016/j.vaccine.2024.06.011. Epub 2024 Jun 15. Vaccine. 2024. PMID: 38879409
-
A Cost-Effectiveness Analysis of the Switch to 20-Valent Pneumococcal Conjugate Vaccine from Lower-Valent Pneumococcal Conjugate Vaccines in the French Pediatric Population.Infect Dis Ther. 2025 Aug 15. doi: 10.1007/s40121-025-01209-z. Online ahead of print. Infect Dis Ther. 2025. PMID: 40815494
-
Immunogenicity and seroefficacy of pneumococcal conjugate vaccines: a systematic review and network meta-analysis.Health Technol Assess. 2024 Jul;28(34):1-109. doi: 10.3310/YWHA3079. Health Technol Assess. 2024. PMID: 39046101 Free PMC article.
-
Vaccines for preventing influenza in healthy adults.Cochrane Database Syst Rev. 2018 Feb 1;2(2):CD001269. doi: 10.1002/14651858.CD001269.pub6. Cochrane Database Syst Rev. 2018. PMID: 29388196 Free PMC article.
References
-
- Moore M.R., Link-Gelles R., Schaffner W., Lynfield R., Holtzman C., Harrison L.H., Zansky S.M., Rosen J.B., Reingold A., Scherzinger K., et al. Effectiveness of 13-valent pneumococcal conjugate vaccine for prevention of invasive pneumococcal disease in children in the USA: A matched case-control study. Lancet Respir. Med. 2016;4:399–406. doi: 10.1016/S2213-2600(16)00052-7. - DOI - PubMed
-
- Centers for Disease Control and Prevention Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among children aged 6–18 years with immunocompromising conditions: Recommendations of the Advisory Committee on Immunization Practices (ACIP) MMWR Morb. Mortal. Wkly. Rep. 2013;62:521–524. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
