

Risk factors and short-term respiratory outcomes associated with unplanned extubations during neonatal intensive care
- PMID: 40873734
- PMCID: PMC12378593
- DOI: 10.3389/fped.2025.1643057
Risk factors and short-term respiratory outcomes associated with unplanned extubations during neonatal intensive care
Abstract
Background: Unplanned extubation (UE) represents an unwanted adverse event in neonatal intensive care. Although skin-to-skin care (SSC) in intubated infants receiving mechanical ventilation (MV) is challenging, its impact on the incidence of UEs has not been reported.
Purpose: To determine the incidence, infant characteristics, and short-term respiratory outcomes of UEs in a unit applying SSC as standard of care also during MV.
Methods: Single-center retrospective cohort study including all infants receiving MV in a Swedish tertiary care center during 2021-2023. UE incidence was calculated per 100 days of MV related to time spent in conventional care (CC) and SSC, using automated chart review of electronic medical records. Pre-defined short-term respiratory outcomes were mode of respiratory support, ventilator settings and fraction of inspired oxygen (FiO2), at 30-120 min post-UE.
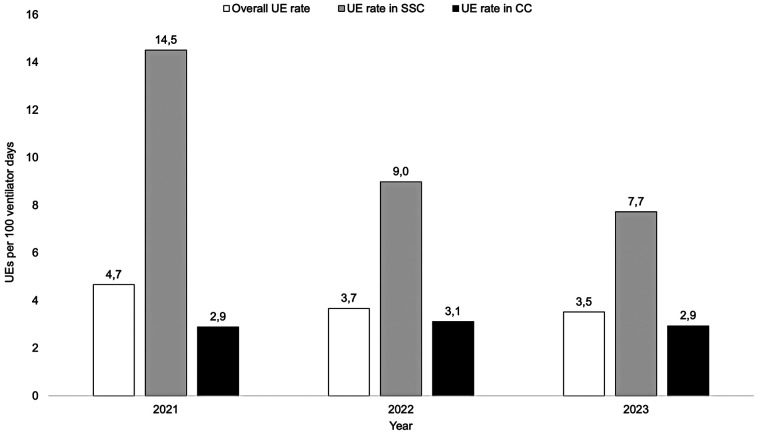
Results: The UE incidence was 3.9 per 100 days of MV (3.0 in CC vs. 10.4 in SSC; p < 0.001). The UE incidence during SSC decreased from 14.5 in 2021, to 7.7 in 2023 (p = 0.07), whereas it remained the same during CC. After UE, 72% infants were reintubated within 120 min, and showed an increased mean FiO2 (0.37 vs. 0.43; p = 0.01).
Conclusions: The number of UEs were high during SSC but decreased during the study period. Reintubation was not required in >25% of all UEs, regardless of type of care. Following UE, an increased need for supplemental oxygen was observed. Safe SSC in mechanically ventilated infants requires experienced staff and increased staff and parental risk awareness.
Keywords: mechanical ventilation; neonatal intensive care; neonate; preterm infant; skin-to-skin care; unplanned extubation.
© 2025 Mannerstedt, Markasz, Karlsson, Pettersson, Blomqvist, Ågren and Sindelar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Sharek PJ, Horbar JD, Mason W, Bisarya H, Thurm CW, Suresh G, et al. Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool to identify harm in north American NICUs. Pediatrics. (2006) 118(4):1332–40. 10.1542/peds.2006-0565 - DOI - PubMed
LinkOut - more resources
Full Text Sources