

Distribution and Surgical Treatment of Corneal Dystrophies Over Eight Decades (1945-2024): An Analysis of Histopathologically Confirmed Cases from a German Center
- PMID: 40874967
- PMCID: PMC12394727
- DOI: 10.1007/s44197-025-00458-y
Distribution and Surgical Treatment of Corneal Dystrophies Over Eight Decades (1945-2024): An Analysis of Histopathologically Confirmed Cases from a German Center
Abstract
Background: Corneal dystrophies are inherited disorders that can lead to significant visual impairment and often require surgical intervention in advanced stages. Fuchs endothelial corneal dystrophy (FECD) is the most frequently diagnosed type in Western countries and remains a leading global indication for corneal transplantation. In contrast, non-Fuchs dystrophies represent a diverse group of less common entities, each with distinct clinical features, surgical considerations, and regional variations in incidence and management. Despite their relevance, long-term data on the full spectrum of corneal dystrophies remain scarce. This study aimed to evaluate the distribution and temporal trends in dystrophy types and associated surgical procedures over eight decades at a tertiary referral center in Germany.
Methods: This retrospective analysis included 3 827 histopathologically confirmed corneal dystrophy specimens identified from an archive of 58 150 ophthalmic specimens collected between 1945 and 2024. Extracted data included dystrophy type, patient age at surgery, sex assigned at birth and associated surgical procedures. Distribution and temporal trends were analyzed descriptively.
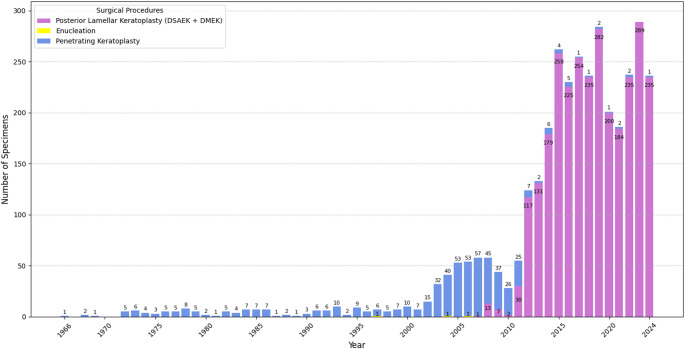
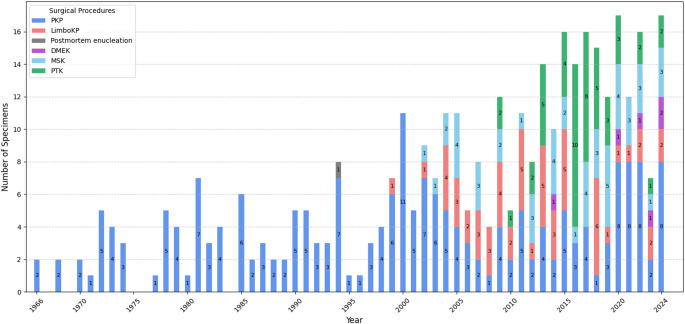
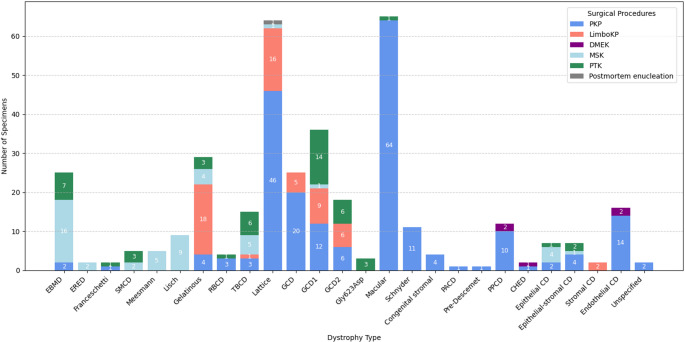
Results: FECD accounted for 90.3% (n = 3 455) of all cases, with a more than 15-fold increase in annual cases between 2003 and 2024. Its surgical management transitioned from exclusive use of penetrating keratoplasty (PKP) to posterior lamellar keratoplasty in over 99% of cases by 2024. Among non-Fuchs dystrophies (n = 372), granular (21.2%), macular (17.5%), and lattice dystrophy (17.2%) were most frequent. These exhibited greater surgical variability, reflecting their heterogeneity across 21 non-Fuchs dystrophy types in this study. Stromal and epithelial-stromal dystrophies were predominantly managed with PKP, whereas superficial epithelial and basement membrane dystrophies were increasingly treated with phototherapeutic or manual superficial keratectomy. Limbo-keratoplasty was introduced in the early 2000s for recurrent subepithelial and epithelial-stromal types.
Conclusion: This study provides unique insights into the type distribution and surgical management of corneal dystrophies over eight decades in a German center, encompassing nearly all IC3D-classified entities. The marked increase in FECD specimen numbers and the shift toward lamellar keratoplasty reflect evolving clinical practices and rising demand on corneal transplantation services. The broader clinical spectrum and procedural diversity among non-Fuchs dystrophies underscore the ongoing need for pathology-specific management strategies tailored to population-specific needs.
Keywords: Cornea; Corneal dystrophies; Histopathology; Keratoplasty; Longitudinal study; Ocular epidemiology; Ophthalmic pathology; Surgical trends; Transplantation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics Approval and Consent to Participate: This retrospective study was approved by the Ethics Committee at the University of Freiburg Medical Center (approval number 25-1067-S1-retro), with a waiver of informed consent, and conducted in accordance with the Declaration of Helsinki. Consent for Publication: Not applicable. Competing Interests: The authors declare no competing interests.
Figures


Similar articles
-
Endothelial keratoplasty versus penetrating keratoplasty for Fuchs endothelial dystrophy.Cochrane Database Syst Rev. 2014 Feb 14;2014(2):CD008420. doi: 10.1002/14651858.CD008420.pub3. Cochrane Database Syst Rev. 2014. PMID: 24526345 Free PMC article.
-
Endothelial keratoplasty versus penetrating keratoplasty for Fuchs endothelial dystrophy.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD008420. doi: 10.1002/14651858.CD008420.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2014 Feb 14;(2):CD008420. doi: 10.1002/14651858.CD008420.pub3. PMID: 21735430 Updated.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Descemet's membrane endothelial keratoplasty is the predominant keratoplasty procedure in Germany since 2016: a report of the DOG-section cornea and its keratoplasty registry.Br J Ophthalmol. 2024 May 21;108(5):646-653. doi: 10.1136/bjo-2022-323162. Br J Ophthalmol. 2024. PMID: 37586835 Free PMC article.
-
Surveillance for Violent Deaths - National Violent Death Reporting System, 50 States, the District of Columbia, and Puerto Rico, 2022.MMWR Surveill Summ. 2025 Jun 12;74(5):1-42. doi: 10.15585/mmwr.ss7405a1. MMWR Surveill Summ. 2025. PMID: 40493548 Free PMC article.
References
-
- Moshirfar M, Bennett P, Ronquillo Y. Corneal Dystrophy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2025 Jan 4]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557865/
-
- Gain P, Jullienne R, He Z, Aldossary M, Acquart S, Cognasse F, et al. Global survey of corneal transplantation and eye banking. JAMA Ophthalmol. 2016;134(2):167–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
