

Lung electrical impedance tomography during positioning, weaning and chest physiotherapy in mechanically ventilated critically ill patients: a narrative review
- PMID: 40877702
- PMCID: PMC12394117
- DOI: 10.1186/s13613-025-01526-z
Lung electrical impedance tomography during positioning, weaning and chest physiotherapy in mechanically ventilated critically ill patients: a narrative review
Abstract
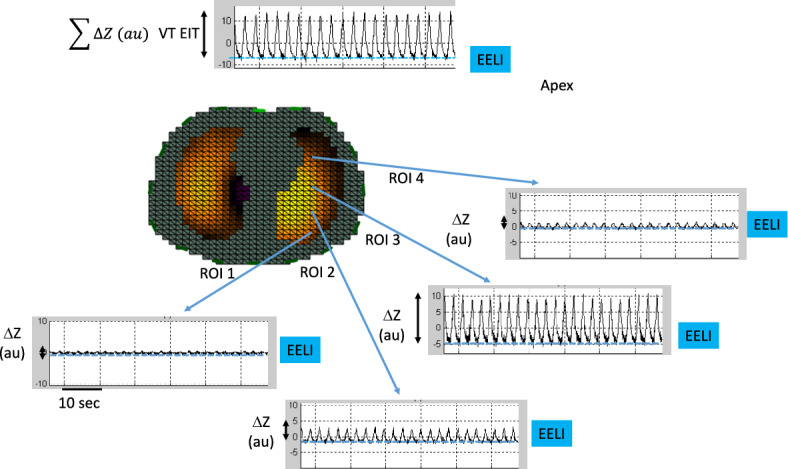
Background: Electrical impedance tomography (EIT) is a non-invasive, radiation free, lung imaging technique of lung ventilation with a low spatial but a high temporal resolution available at the bedside. Lung perfusion, and hence ventilation-to-perfusion ratios, can also be assessed with EIT. Most of the EIT studies in intensive care units (ICU) are dedicated to positive end expiratory pressure selection in patients with acute respiratory distress syndrome receiving invasive mechanical ventilation. This narrative review explores the use of EIT during change in body position, weaning and chest physiotherapy in adult intubated ICU patients.
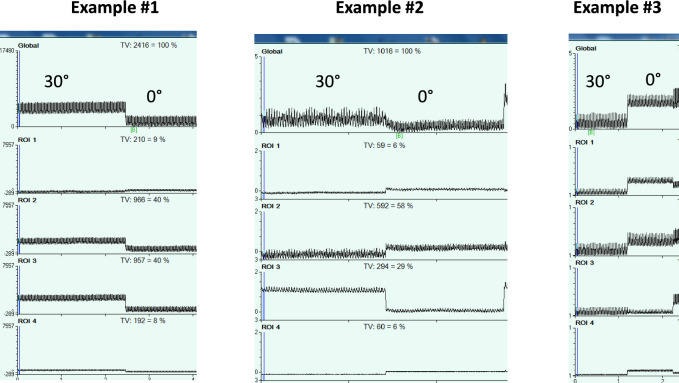
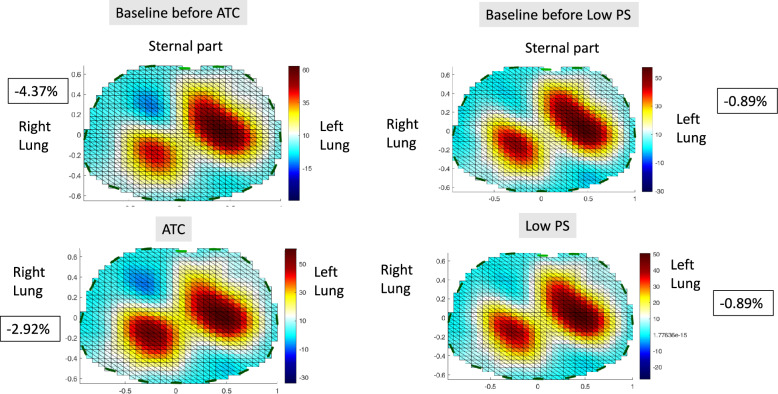
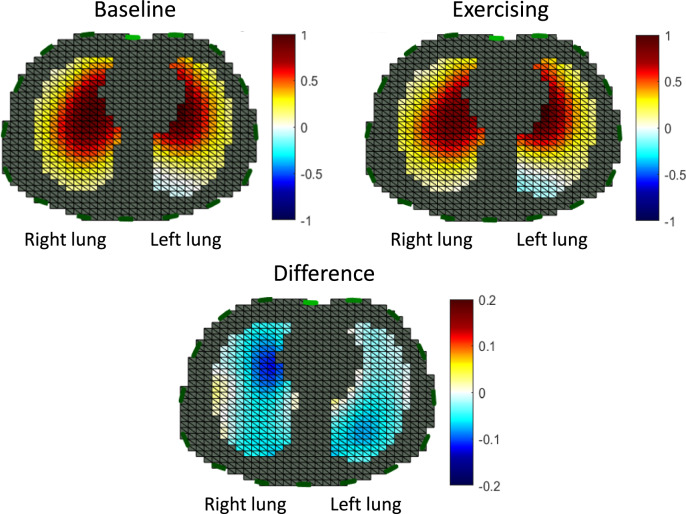
Main body: EIT findings confirm a better ventilation and the persistence of lung perfusion in the dorsal lung regions in prone as compared to supine position. However, the response of the ventilation distribution to prone is heterogeneous across patients. For the weaning, global inhomogeneity index, end-expiratory lung impedance, absolute ventral-to-dorsal difference of the change in lung impedance and temporal skew of aeration had a good performance to predict spontaneous breathing trial (SBT) failure in some observational studies. Pendelluft that measures the risk of overstretching in dependent lung regions can only be assessed with EIT. It occurs frequently during weaning and is associated with poor patient outcome. However, its performance to predict SBT failure was moderate. Randomized controlled trials comparing SBT techniques did not find a difference in EIT indexes. The effects of other body positions and chest physiotherapy have been less investigated with EIT.
Conclusion: EIT offers the possibility to monitor lung ventilation and perfusion at the bedside and hence to deliver a personalized ventilatory management. Further designed EIT studies coupled with measurement of lung aeration and patient breathing effort are warranted during weaning to check if the technique is useful to clinical outcome. The same is true regarding the optimal use of body position including prone, and of chest physiotherapy in ICU patients.
Keywords: Chest physiotherapy; Clearing airways secretion; Electrical impedance tomography; Intensive care unit; Lateral position; Positioning; Prone position; Semi-recumbent position; Weaning.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: None.
Figures
References
-
- Piraino T. An introduction to the clinical application and interpretation of electrical impedance tomography. Respir Care. 2022;67:721–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
