

Geographic and socioeconomic differences in potentially inappropriate medication among older adults - applying a simplified analysis of individual heterogeneity and discriminatory accuracy (AIHDA) for basic comparisons of healthcare quality
- PMID: 40877856
- PMCID: PMC12395699
- DOI: 10.1186/s12913-025-13335-y
Geographic and socioeconomic differences in potentially inappropriate medication among older adults - applying a simplified analysis of individual heterogeneity and discriminatory accuracy (AIHDA) for basic comparisons of healthcare quality
Abstract
Background: Monitoring of healthcare quality is typically focused on differences between group averages in relation to a desirable benchmark. However, we need to consider (i) the existence of interconnected socioeconomic axes of inequality like age, sex, income, and country of birth and (ii) individual heterogeneity around group averages. Additionally, (iii) we need clear criteria to quantify group differences. By applying the framework analysis of individual heterogeneity and discriminatory accuracy (AIHDA) on an established quality indicator (potentially inappropriate medication (PIM)), we illustrate how to achieve these improvements and how to avoid both unnecessary group stigmatization and false expectations.
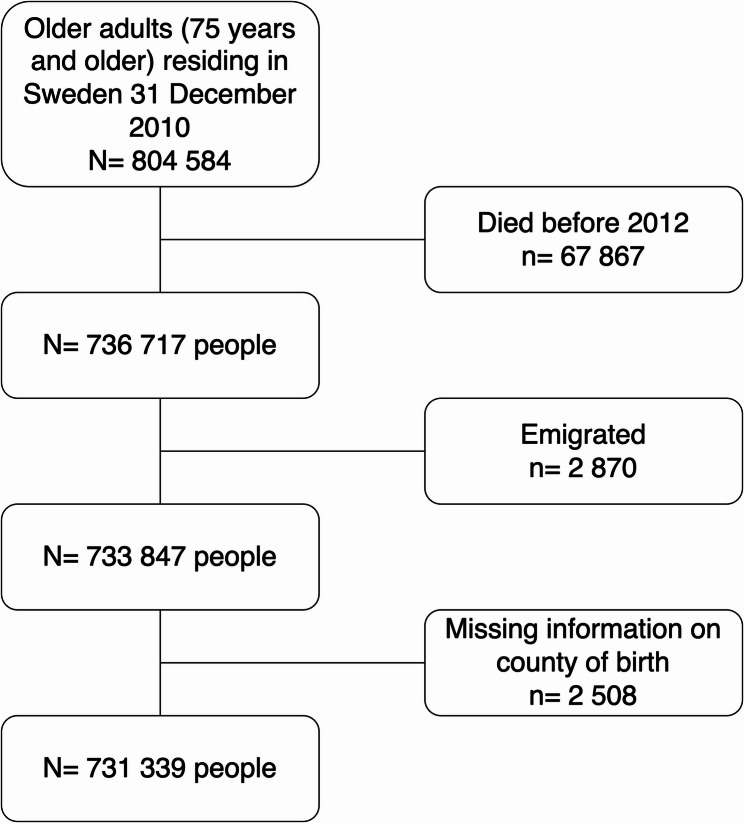
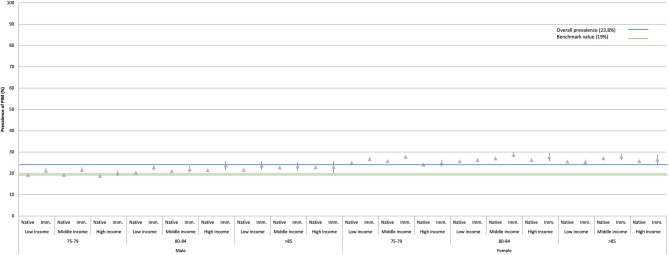
Methods: We analyzed 731,339 individuals, ≥ 75-year-old belonging to 36 socioeconomic strata defined by the intersection of age, sex, income, and country of birth, who were alive and residing in the 21 regions Swedish during 2011. We calculated PIM prevalences and evaluate the discriminatory accuracy (DA) of the socioeconomic and geographical group differences using the area under the ROC curve (AUC). The benchmark value was defined as a prevalence of 19%.
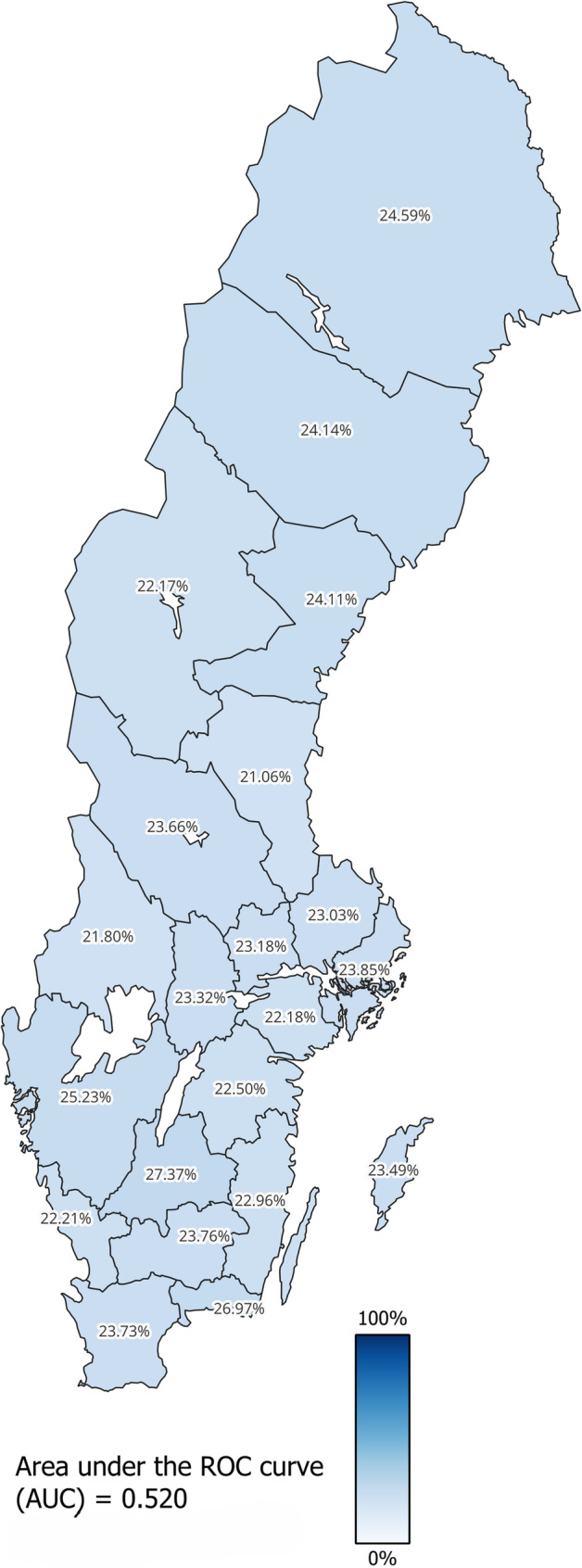
Results: In Sweden, the prevalence of PIM was 24% among ≥ 75-year-olds and regionally it ranged between 21% and 27%. Immigrant 80-84-year-old women with low income had the highest prevalence (29%). All strata including women had higher prevalence than those including men. However, the regional (AUC = 0.520) and socioeconomic (AUC = 0.544) differences were very small. For instance, in the five socioeconomic strata with the lowest prevalence there were about 8,000 more cases of PIM than in the five strata with the highest prevalence of PIM.
Conclusion: The prevalence of PIM was higher than the desired benchmark value. There were disparities between group averages, but overall, the regional and socioeconomic differences were very small as informed by their low AUC values. Therefore, interventions to reduce PIM in Sweden should be universal rather than only targeted at the regions and socioeconomic strata with the highest PIM prevalence.
Keywords: Epidemiological methods; Health care quality assessment; Health services evaluation; MeSH; Pharmacoepidemiology; Social epidemiology.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval for research involving human participants was given by Regional ethics committee Lund (ID 2014/856). Informed consent was not necessary according to the Regional ethics committee because of the nature of the register study. The database was approved by National board of health and welfare (ID 9542/2015) and by Statistics Sweden (ID 231424/878144-5). Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Trust in healthcare and perceived discrimination in Sweden: a fixed effects analysis of individual heterogeneity and discriminatory accuracy.Front Public Health. 2025 Jun 11;13:1557921. doi: 10.3389/fpubh.2025.1557921. eCollection 2025. Front Public Health. 2025. PMID: 40567967 Free PMC article.
References
-
- Welfare SNBoHa. God vård – om ledningssystem för kvalitet och patientsäkerhet i hälso- och sjukvården. 2006. Contract No.: Artikelnummer: 2006-101-2.
-
- Swedish. healthcare act 2017:30.
-
- Heurgren M, Åberg A, Köster M, et al. Performance indicators in Swedish Health Care. BMC Health Serv Res. 2007;7(Suppl 1):A10. 10.1186/1472-6963-7-S1-A10.
-
- Swedish Association of Local Authorities and Regions. Öppna jämförelser av hälso- och sjukvårdens kvalitet och effektivitet. 2009.
-
- Sorman H. [Open comparisons of health care: one of the most important contributions to modernization of health care]. Lakartidningen. 2010;107(32–33):1828–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
