

PD-1+ NK cell subsets in high grade serous ovarian cancer: an indicator of disease severity and a target for combined immune-checkpoint blockade
- PMID: 40877861
- PMCID: PMC12395815
- DOI: 10.1186/s13046-025-03508-2
PD-1+ NK cell subsets in high grade serous ovarian cancer: an indicator of disease severity and a target for combined immune-checkpoint blockade
Abstract
Background: Ovarian cancer (OC) is the fifth leading cause of cancer-related death among women, with High-Grade Serous Ovarian Carcinoma (HGSC) representing the most aggressive and prevalent subtype. Despite promising results in other malignancies, immune checkpoint blockade has shown limited efficacy in HGSC, highlighting the need for alternative immunotherapeutic targets.
Methods: We conducted an integrated analysis combining multiparametric flow cytometry, RNA sequencing, multiplex immunohistochemistry, and functional assays to characterize NK cells isolated from peripheral blood, peritoneal fluid, primary tumor tissue, and metastases in 60 HGSC patients.
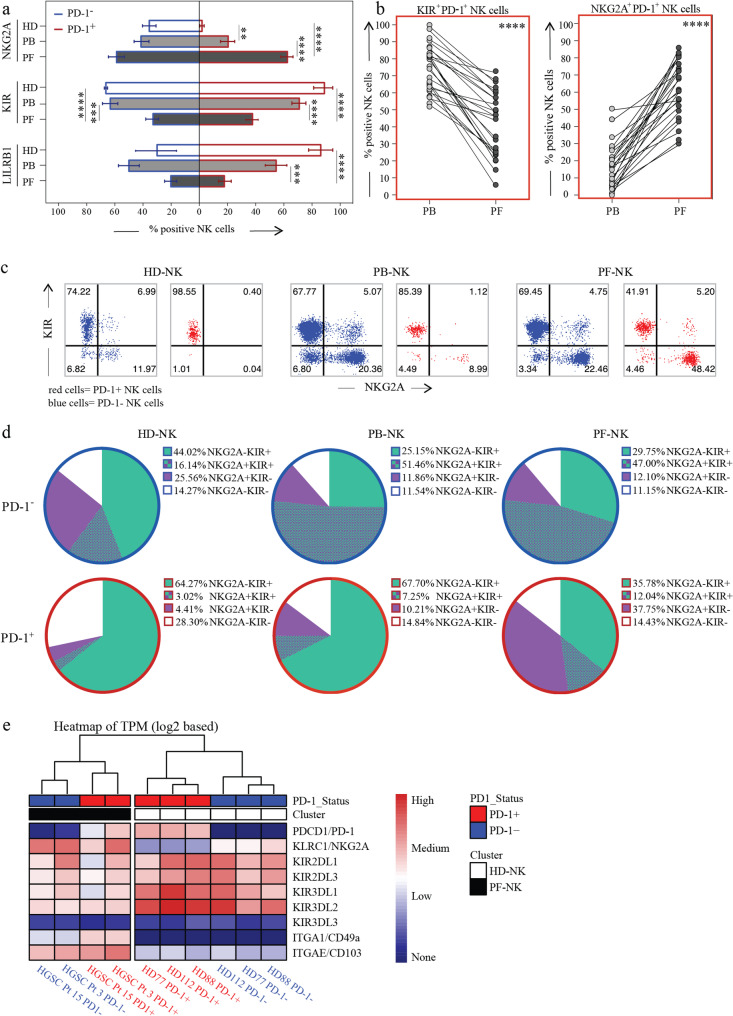
Results: We identified a distinct population of PD-1⁺ NK cells enriched in HGSC tumors and metastatic sites but absent in healthy donors. These cells, characterized by a CD56dimNKG2A⁺KIR⁺/⁻NKp46⁺CD57low phenotype, displayed impaired cytotoxicity against autologous HGSC targets, correlating with poorer prognosis. Crucially, this dysfunction was reversible upon combined blockade of PD-1/PD-L1, NKG2A, and KIRs. Spatial and molecular profiling revealed that these cells localize within PD-L1⁺/HLA-E⁺ tumor niches, suggesting that immune suppression is spatially and molecularly coordinated. Transcriptomic analysis confirmed their altered functional state and highlighted actionable checkpoint targets.
Conclusions: Our findings uncover a previously underappreciated population of dysfunctional PD-1⁺ NK cells in HGSC and demonstrate that their suppression is reversible through combinatorial checkpoint inhibition. These insights support the development of spatially-informed, NK-targeted immunotherapies for HGSC patients, particularly those resistant to T cell-based strategies.
Supplementary Information: The online version contains supplementary material available at 10.1186/s13046-025-03508-2.
Keywords: Immune checkpoint; Immunotherapy; Natural killer cells; Ovarian cancer; Programmed cell death 1 receptor; Tumor escape; Tumor infiltrating.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was carried out in accordance with the recommendations of the ethical standards of the institutional and/or national research committee. The protocol was approved by the ethics committee of the Liguria Region, Genova, Italy (n. 326/2018 and n127/2022-DB id12223 for OC patients and n. 39/2012 for healthy donors, by Spedali Civili of Brescia institutional ethical board (n. 1892/2010 for OC patients). All subjects gave written informed consent in accordance with the Declaration of Helsinki. Consent for publication: All authors have approved the submitted version. Competing interests: Eric Vivier and Pascale Andrè are employees of Innate Pharma, all other authors present no Conflicts of Interest.
Figures







References
Grants and funding
- Post Doctoral Fellowship Year 2024-2025/Fondazione Umberto Veronesi
- 26037/Fondazione AIRC per la ricerca sul cancro ETS
- 21147/Fondazione AIRC per la ricerca sul cancro ETS
- 21147/Fondazione AIRC per la ricerca sul cancro ETS
- 21147/Fondazione AIRC per la ricerca sul cancro ETS
- 2022FFALH_001/PRIN MIUR 2022
- TILC, grant agreement No. 694502, grant agreement No. 875102 - MInfla-Tilc/European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program
- TILC, grant agreement No. 694502, grant agreement No. 875102 - MInfla-Tilc/European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program
- ANR-17-RHUS-0007/the Agence Nationale de la Recherche including the PIONEER Project
- ANR-17-RHUS-0007/the Agence Nationale de la Recherche including the PIONEER Project
- KFS-5250-02-2021/Swiss Cancer League
- KFS-5250-02-2021/Swiss Cancer League
- P2022PKFNB/PRIN-MIUR PNRR 2022
- 2022YCKH7K/PRIN-MIUR 2022
LinkOut - more resources
Full Text Sources
Research Materials
