

Hyperlipidemia drives tumor growth in a mouse model of obesity-accelerated breast cancer growth
- PMID: 40877972
- PMCID: PMC12395885
- DOI: 10.1186/s40170-025-00407-0
Hyperlipidemia drives tumor growth in a mouse model of obesity-accelerated breast cancer growth
Abstract
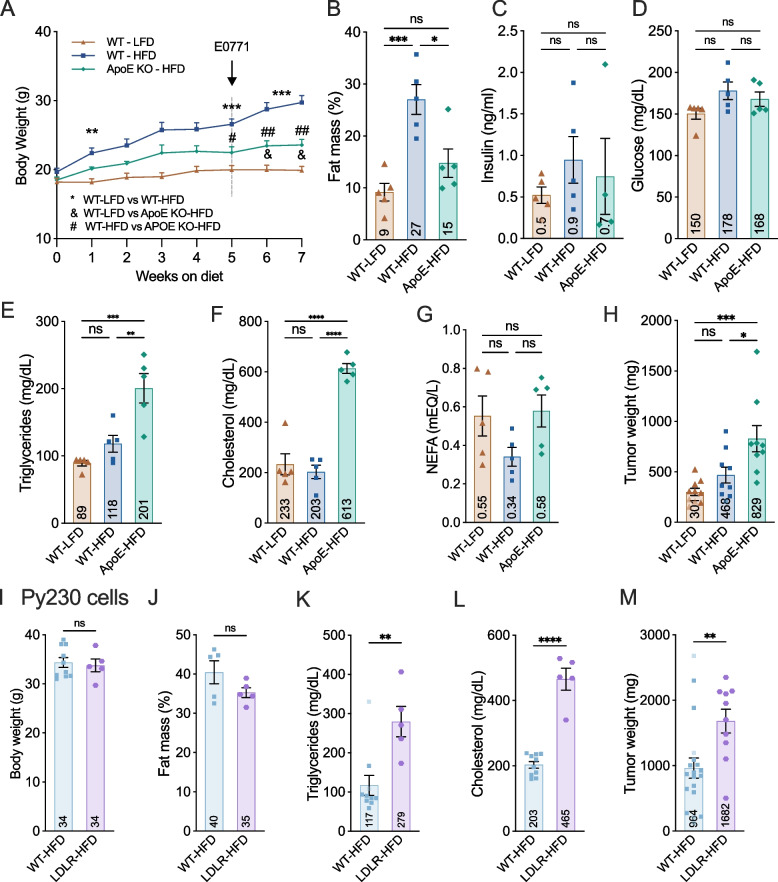
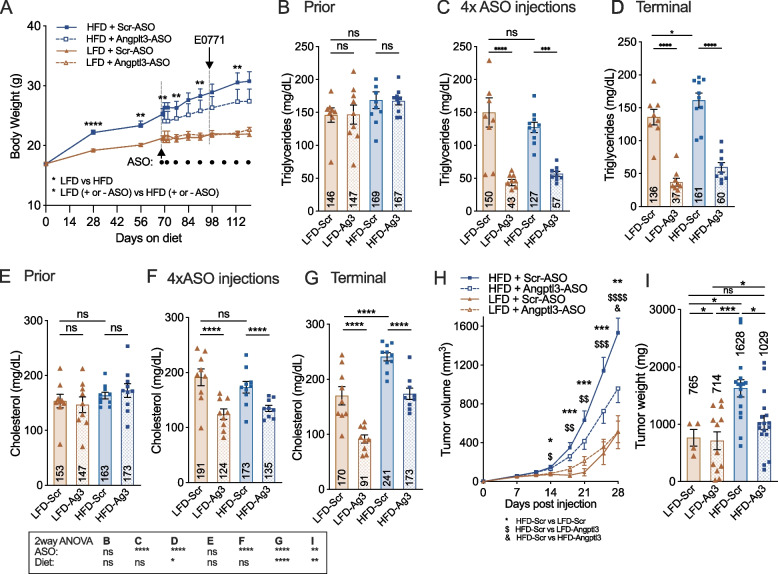
Obesity is an established risk factor for breast cancer (BC), yet the specific mechanisms driving this association remain unclear. Dysregulated lipid metabolism has emerged as a key factor in cancer cell biology, and, while obesity is often accompanied by hyperlipidemia, the isolated impact of elevated lipid levels on BC growth has not been experimentally tested. Using the E0771 and Py230 orthotopic models of obesity-accelerated BC growth in immune-competent mice, we investigated the role of systemic lipids on tumor growth. Combining dietary and genetic mouse models, we show that elevated circulating lipids are sufficient to accelerate BC tumor growth even in the absence of obesity or alterations in blood glucose and/or insulin levels. Pharmacological lowering of systemic lipid levels attenuates BC growth in obese mice, suggesting a direct role for lipids in fueling tumor expansion. Notably, we also show that weight loss alone, without a corresponding reduction in lipid levels such as that induced by a ketogenic diet, fails to protect against BC, highlighting the necessity of targeting lipid metabolism in obesity-associated BC. Our findings establish hyperlipidemia as a critical driver of BC progression and suggest that lipid-lowering interventions may be a promising strategy to mitigate BC risk in individuals with obesity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
Hyperlipidemia drives tumor growth in a mouse model of obesity-accelerated breast cancer growth.bioRxiv [Preprint]. 2025 Feb 13:2025.02.10.637542. doi: 10.1101/2025.02.10.637542. bioRxiv. 2025. PMID: 39990404 Free PMC article. Preprint.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Bluher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–98. 10.1038/s41574-019-0176-8. Epub 2019/03/01 PubMed PMID: 30814686. - PubMed
-
- Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K. International Agency for Research on Cancer Handbook Working G Body Fatness and Cancer-Viewpoint of the IARC Working Group. N Engl J Med. 2016;375(8):794–8. 10.1056/NEJMsr1606602. PubMed PMID: 27557308; PMCID: PMC6754861 Epub 2016/08/25. - PMC - PubMed
-
- Heer E, Harper A, Escandor N, Sung H, McCormack V, Fidler-Benaoudia MM. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study. Lancet Glob Health. 2020;8(8):e1027–37. 10.1016/S2214-109X(20)30215-1. PubMed PMID: 32710860 Epub 2020/07/28. - PubMed
-
- Munsell MF, Sprague BL, Berry DA, Chisholm G, Trentham-Dietz A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol Rev. 2014;36(1):114–36. 10.1093/epirev/mxt010. PubMed PMID: 24375928; PMCID: PMC3873844 Epub 2014/01/01. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
