

Interventional Psychiatry and Emerging Treatments for Posttraumatic Stress Disorder (PTSD): A Systematic Review
- PMID: 40879152
- PMCID: PMC12410247
- DOI: 10.5152/pcp.2025.241027
Interventional Psychiatry and Emerging Treatments for Posttraumatic Stress Disorder (PTSD): A Systematic Review
Abstract
Background: Posttraumatic stress disorder (PTSD) is a severe, often difficult-to-treat condition, highlighting the need for innovative therapies. Interventional treatments, including neuromodulation, rapid-acting pharmacotherapies such as intravenous ketamine (IV-KET) and esketamine (ESK), and emerging psychedelic-assisted psychotherapies, offer promising solutions. This systematic review evaluates the efficacy, safety, and future research priorities of these treatments for PTSD.
Methods: A search strategy was implemented across 3 electronic databases. Peer-reviewed articles written in English that focused on interventional psychiatry treatments for adult patients with PTSD were included.
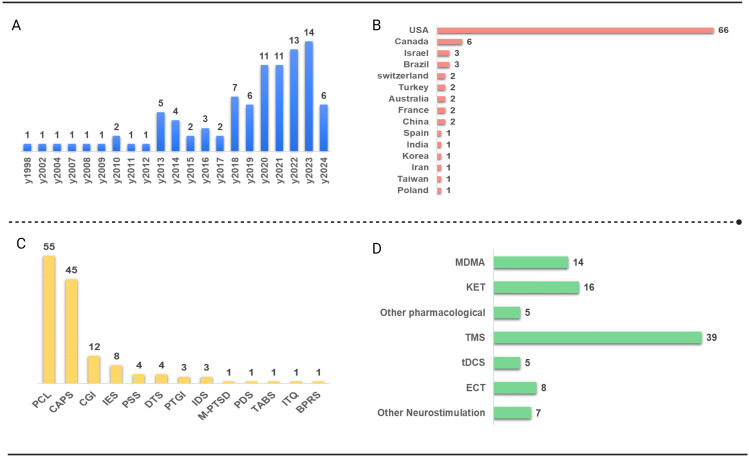
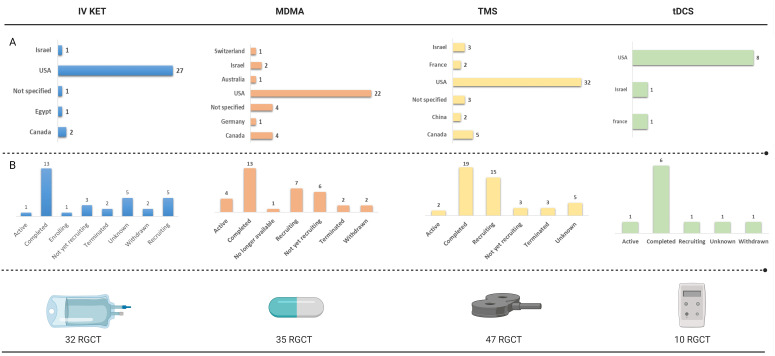
Results: The systematic review encompassed 94 studies, including 39 on transcranial magnetic stimulation (TMS), 8 on IV-KET, 3 on intranasal esketamine (IN-ESK), 4 on intravenous ketamine (IV-KET) assisted therapy (KET-AT), 1 on esketamine (ESK) assisted therapy (ESK-AT), and 14 on 3,4-methylenedioxymethamphetamine assisted therapy (MDMA-AT). Randomized controlled trials demonstrated response rates of 12.5%-80% for TMS, 17%-67% for IV-KET, and 50%-87% for MDMA. Additional treatments reviewed included Electroconvulsive Therapy, transcranial direct current stimulation, and other pharmacological and neurostimulation treatments. Most treatments were well tolerated, with only mild, transient adverse effects.
Conclusions: This review highlights the heterogeneity in efficacy, safety, and tolerability across neuromodulation and pharmacologic treatments for PTSD. Variability in response rates reflects differences in patient populations, protocols, and comorbidities. While repetitive TMS, IV-KET, ESK, KET-AT, and MDMA-AT show symptom improvement, sustained efficacy varies, underscoring the need for maintenance strategies. Although direct evidence on stage-specific approaches is limited, these methods, guided by neuroscience-based nomenclature, may improve therapeutic precision, especially in complex cases.
Conflict of interest statement
Figures



References
-
- Çelik YS, Efe A, Aydos BS, Akbas Aliyev ES, Cura M, Harputlu Yamak Y, Demirkol Tunca R, Kaşak M, Öztürk Y. Psychiatric manifestations following the 2023 kahramanmaraş earthquakes: a focus on children and adolescents. Psychiatry Clin Psychopharmacol. 2024;34(4):302 310. (doi: 10.1007/s40596-014-0050-x) - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources