

5-year clinical outcome of the ESTOIH trial comparing the short-bite versus large-bite technique for elective midline abdominal closure
- PMID: 40879826
- PMCID: PMC12397119
- DOI: 10.1007/s10029-025-03459-9
5-year clinical outcome of the ESTOIH trial comparing the short-bite versus large-bite technique for elective midline abdominal closure
Abstract
Background: The short-bite technique for fascial closure after midline laparotomy has been shown to reduce the incidence of incisional hernias one year postoperatively compared to the traditional large-bite technique. However, most studies evaluating this approach have been limited to a one-year follow-up period. Initiated in 2013, the ESTOIH trial is the only randomised controlled study to include both 3-year and 5-year follow-up data. The 3-year clinical outcomes have been previously published. Herein, we report for the first time the 5-year results regarding the incisional hernia rate using the small-bite technique compared to the large-bite technique for elective midline closure.
Methods: The ESTOIH study was designed as a prospective, multicentre, parallel, double-blind, randomised controlled study of primary elective midline closure. Patients were randomly assigned to receive either the small-bite or large-bite technique to close the fascia using an ultra-long-term, absorbable, elastic, monofilament suture named Monomax® based on poly-4-hydroxybutyrate. A planned 5-year follow-up was conducted, including ultrasound/radiological imaging to assess incisional hernia development as a key outcome parameter for the long-term effectiveness of the procedure.
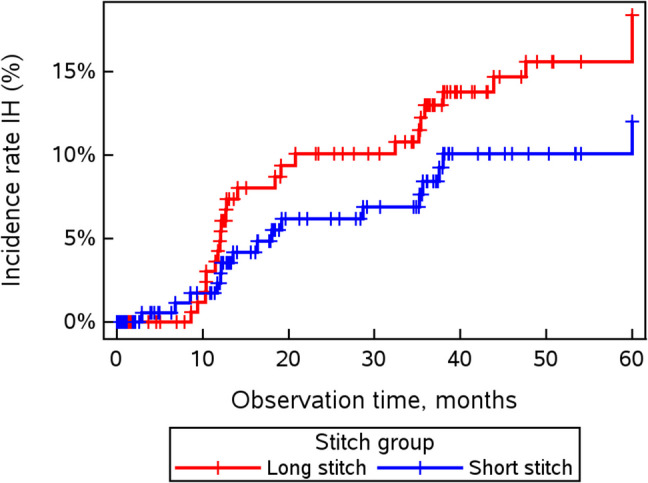
Results: In total, 362 patients were included in the 5-year ITT analysis (175 and 187 patients in the short-bite and large-bite groups, respectively). The incisional hernia rate increased in the short-bite group from 7.58% to 9.14% (p = 0.58) and in the large-bite group from 10.45% to 13.90% (p = 0.30) after 5 years compared to 3 years postoperatively. The incisional hernia rate in the short-stitch group was low, at 9.14% five years after surgery; however, the difference between the two treatment groups (short vs. long) was not significant at 5 years (OR 1.60, 95% CI [0.82-3.10]; p = 0.155).
Conclusion: The previously observed increase in incisional hernias from 1 to 3 years postoperatively continued to 5 years in both stitch groups. The incisional hernia rate in the long-stitch group appeared to be higher at every time point than that in the short-stitch group. Using the short-bite technique in combination with an extra-long-term absorbable, elastic, monofilament poly-4-hydroxybutyrate suture, it may be possible to achieve a very low incisional hernia rate in the long-term follow-up.
Trial registry: NCT01965249, registered October 18, 2013.
Keywords: Abdominal wall closure; Incisional hernia; Laparotomy; Randomised controlled trial; Suture bite technique; Suture stitch technique.
© 2025. The Author(s).
Figures


References
-
- Nunoo-Mensah JW, Rosen M, Chan LS, Wasserberg N, Beart RW (2009) Prevalence of intra-abdominal surgery: what is an individual’s lifetime risk? South Med J 102(1):25–29. 10.1097/SMJ.0b013e318182575b - PubMed
-
- Höer J, Lawong G, Klinge U, Schumpelick V (2002) Factors influencing the development of incisional hernia: a retrospective study of 2,983 laparotomy patients over a period of 10 years. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen 73(5):474–480 - PubMed
-
- Fink C, Baumann P, Wente MN, Knebel P, Bruckner T, Ulrich A et al (2014) Incisional hernia rate 3 years after midline laparotomy. J Br Surg 101(2):51–54. 10.1002/bjs.9364 - PubMed
-
- Diener MK, Voss S, Jensen K, Büchler MW, Seiler CM (2010) Elective midline laparotomy closure: the INLINE systematic review and meta-analysis. Ann Surg 251(5):843–856. 10.1097/SLA.0b013e3181d973e4 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
