

Effects of different vitamins on individuals with septic shock: a Bayesian NMA of RCTs
- PMID: 40880742
- PMCID: PMC12380562
- DOI: 10.3389/fnut.2025.1566422
Effects of different vitamins on individuals with septic shock: a Bayesian NMA of RCTs
Abstract
Objective: To compare the effects of different vitamins on patients with septic shock (SS) through Bayesian network meta-analysis.
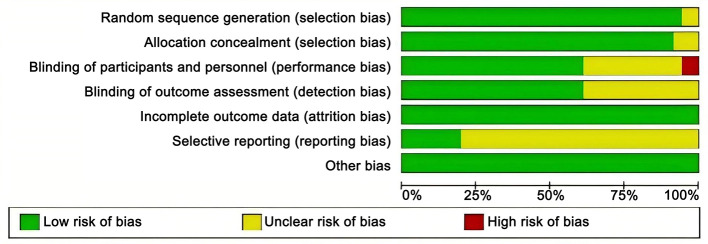
Methods: Randomized controlled trials (RCTs) on vitamins for septic shock patients were retrieved from PubMed, Embase, Cochrane Library, Web of Science, etc. The retrieval time was set from the establishment of the database to May 20, 2024. All relevant studies on vitamin treatment for septic shock were retrieved and screened according to the established inclusion and exclusion criteria. Intensive care unit (ICU) length of stay, mechanical ventilation time, Sequential Organ Failure Assessment (SOFA) scores after 24 h, total hospital stay, and 28-day mortality were used as outcome measures. The quality of the included studies was evaluated for risk of bias, and R software was used for data analysis.
Results: A total of 36 articles were included in the analysis, covering 4,473 patients with septic shock. The vitamins included vitamin B (VB), vitamin C (VC), vitamin D (VD), vitamin E (VE), hydroxocobalamin (HYD), and vitamin combinations such as hydrocortisone plus vitamin C plus vitamin B (HYDVCVB), vitamin D plus probiotics (VDP), vitamin C plus vitamin B (VCVB), and hydrocortisone plus vitamin C (HYDVC). The network meta-analysis results showed that in terms of ICU length of stay, VD was superior to the control group [mean difference (MD) = 4.57, 95% CI (1.01, 9.69)] and HYDVCVB [MD = 5.4, 95% CI (0.51, 11.66)], with statistically significant differences. In terms of mechanical ventilation time, VC, VD, VCVB, and HYDVCVB showed no statistically significant differences compared to the control group. Regarding the SOFA score after 24 h, VDP was superior to the control group [MD = 2.98, 95% CI (0.27, 5.62)], as well as HYDVCVB [MD = 3.32, 95% CI (0.59, 6.04)], VB [MD = 2.96, 95% CI (0.18, 5.67)], VC [MD = 2.91, 95% CI (0.17, 5.57)], VCVB [MD = 3.18, 95% CI (0.31, 5.9)], and VD [MD = 2.91, 95% CI (0.05, 5.71)], with statistically significant differences. In terms of total hospital stay, VD was superior to the control group [MD = 7.61, 95% CI (2.59, 12.63)], as well as HYDVCVB [MD = 7.71, 95% CI (2.55, 12.9)], VB [MD = 7.6, 95% CI (0.84, 14.39)], VC [MD = 9.93, 95% CI (3.9, 15.92)], and VCVB [MD = 8.1, 95% CI (1.79, 14.41)], with statistically significant differences. Regarding 28-day mortality, VB, VC, VD, VDP, VCVB, HYDVCVB showed no statistically significant differences compared to the control group.
Conclusion: In patients with septic shock, the use of VD shows certain advantages in reducing ICU length of stay and total hospital length of stay. Moreover, its combination with probiotics may help reduce the SOFA scores after 24 h. However, these interventions have not significantly impacted 28-day mortality or mechanical ventilation time.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, PROSPERO: CRD42024599094.
Keywords: network meta-analysis; septic shock; shock; vitamin D; vitamins.
Copyright © 2025 Tian, Long, Li, Liang, Sun, Song, Yue, Shen, Zhao and Ren.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Hager DN, Hooper MH, Bernard GR, Busse LW, Ely EW, Fowler AA, et al. The vitamin C, thiamine and steroids in sepsis (VICTAS) protocol: a prospective, multi-center, double-blind, adaptive sample size, randomized, placebo-controlled, clinical trial. Trials. (2019) 20:1–16. 10.1186/s13063-019-3254-2 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous