

Impact of Parental or First-Degree Family History of Diabetes on Diabetes Incidence and Progression During Long-term Follow-up in the Diabetes Prevention Program Outcomes Study
- PMID: 40882001
- PMCID: PMC12451838
- DOI: 10.2337/dc25-0633
Impact of Parental or First-Degree Family History of Diabetes on Diabetes Incidence and Progression During Long-term Follow-up in the Diabetes Prevention Program Outcomes Study
Abstract
Objective: To determine the effects of first-degree family history of diabetes on diabetes incidence in Diabetes Prevention Program (DPP) and Diabetes Prevention Program Outcomes Study (DPPOS) participants.
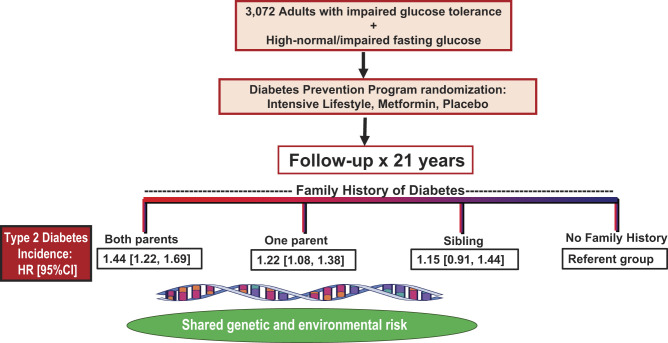
Research design and methods: In the DPP, adults with prediabetes were randomized to an intensive lifestyle intervention, metformin, or placebo and followed for incident diabetes. On study completion 88% of eligible DPP participants reenrolled in DPPOS for long-term follow-up. The present analysis includes all 3,072 participants with family history information through DPPOS, with a median follow-up of 21 years (1,975 had parental history of diabetes [PH] [312 biparental, 947 maternal, 716 paternal], 226 had only sibling history [SH], and 871 denied any family history). The primary outcome is incident diabetes based on American Diabetes Association criteria, with adjustment for demographic and clinical variables, DPP randomization arm, and polygenic risk score (PRS).
Results: Adjusted hazard ratio (HR) was 1.21 (95% CI 1.06, 1.38) for any family history, 1.19 (1.04, 1.35) for PH, and 1.15 (0.91, 1.44) for SH. Biparental history conferred greater hazard (HR 1.44 [95% CI 1.22, 1.69]) than maternal (1.22 [1.08, 1.38]) or paternal (1.22 [1.08, 1.39]) diabetes history alone. PRS explained 32% of the association of any family history with diabetes risk.
Conclusions: PH increased type 2 diabetes risk after DPP treatment group was controlled for. That effect was only partially explained by PRS, suggesting that rare gene variants, familial, and environmental factors may contribute to type 2 diabetes risk in people with prediabetes.
© 2025 by the American Diabetes Association.
Conflict of interest statement
Figures


References
-
- Centers for Disease Control and Prevention . National Diabetes Statistics Report. Accessed 29 June 2025. Available from https://www.cdc.gov/diabetes/php/data-research/index.html
-
- Dal Canto E, Ceriello A, Rydén L, et al. Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol 2019;26(2 Suppl.):25–32 - PubMed
-
- Parker ED, Lin J, Mahoney T, et al. Economic costs of diabetes in the U.S. in 2022. Diabetes Care 2024;47:26–43 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK048375/DK/NIDDK NIH HHS/United States
- DK-55564/National Institutes of Health (NIH)
- DK-55433/National Institutes of Health (NIH)
- U01 DK098246/DK/NIDDK NIH HHS/United States
- U01 DK048339/DK/NIDDK NIH HHS/United States
- U01 DK048375/NH/NIH HHS/United States
- U01 DK048381/NH/NIH HHS/United States
- U01 DK048377/DK/NIDDK NIH HHS/United States
- U01 DK048411/NH/NIH HHS/United States
- U01 DK048407/DK/NIDDK NIH HHS/United States
- U01 DK048437/DK/NIDDK NIH HHS/United States
- U01 DK048406/DK/NIDDK NIH HHS/United States
- U01 DK094176/DK/NIDDK NIH HHS/United States
- U01 DK048412/DK/NIDDK NIH HHS/United States
- U01 DK048434/DK/NIDDK NIH HHS/United States
- U01 DK048400/NH/NIH HHS/United States
- U01 DK048380/NH/NIH HHS/United States
- U01 DK048437/NH/NIH HHS/United States
- U01 DK048413/DK/NIDDK NIH HHS/United States
- R01 DK128129/DK/NIDDK NIH HHS/United States
- U01 DK048514/NH/NIH HHS/United States
- U19 AG078558/AG/NIA NIH HHS/United States
- U01 DK048404/NH/NIH HHS/United States
- U01 DK048397/NH/NIH HHS/United States
- U01 DK048397/DK/NIDDK NIH HHS/United States
- R01 DK067269/DK/NIDDK NIH HHS/United States
- U01 DK048381/DK/NIDDK NIH HHS/United States
- U01 DK048413/NH/NIH HHS/United States
- U01 DK048514/DK/NIDDK NIH HHS/United States
- U01 DK048485/DK/NIDDK NIH HHS/United States
- U01 DK048411/DK/NIDDK NIH HHS/United States
- U01 DK048443/DK/NIDDK NIH HHS/United States
- U01 DK048349/NH/NIH HHS/United States
- U01 DK048380/DK/NIDDK NIH HHS/United States
- U01 DK048489/NH/NIH HHS/United States
- U01 DK048400/DK/NIDDK NIH HHS/United States
- U01 DK048468/DK/NIDDK NIH HHS/United States
- U01 DK048412/NH/NIH HHS/United States
- K23 HL153774/HL/NHLBI NIH HHS/United States
- U01 DK048387/DK/NIDDK NIH HHS/United States
- U01 DK048468/NH/NIH HHS/United States
- U01 DK048377/NH/NIH HHS/United States
- U01 DK048407/NH/NIH HHS/United States
- U01 DK048404/DK/NIDDK NIH HHS/United States
- U01 DK048485/NH/NIH HHS/United States
- U01 DK048434/NH/NIH HHS/United States
- U01 DK048443/NH/NIH HHS/United States
- U01 DK048489/DK/NIDDK NIH HHS/United States
- U01 DK048349/DK/NIDDK NIH HHS/United States
- U01 DK048339/NH/NIH HHS/United States
- U01 DK048406/NH/NIH HHS/United States
- U01 DK048387/NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
