

Transcatheter aortic valve implantation (TAVI) planning CT on 8-cm detector scanners: Proper dose control by combined use of two deep-learning reconstruction algorithms
- PMID: 40883100
- PMCID: PMC12396921
- DOI: 10.1002/acm2.70224
Transcatheter aortic valve implantation (TAVI) planning CT on 8-cm detector scanners: Proper dose control by combined use of two deep-learning reconstruction algorithms
Abstract
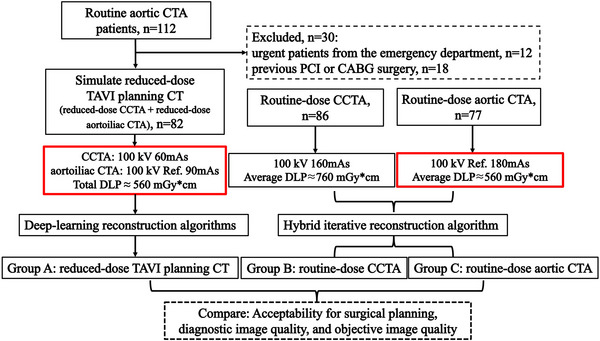
Purpose: To explore the feasibility of transcatheter aortic valve implantation (TAVI) planning computed tomography (CT) on single-source 8-cm detector scanners with proper dose control by using two deep-learning reconstruction algorithms.
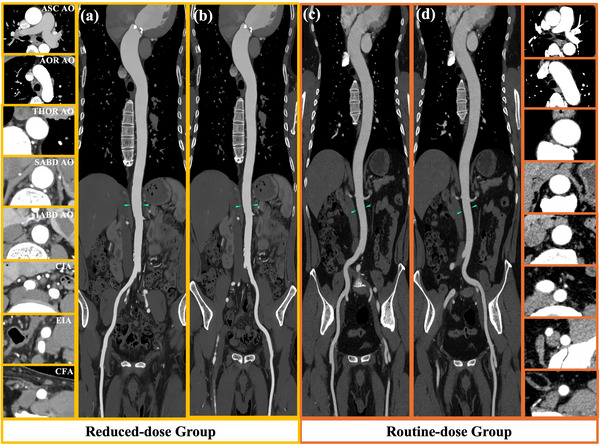
Methods: Reduced-dose TAVI planning CT was simulated by replacing routine aortic CT angiography (CTA) with a reduced-dose aortic CTA and a reduced-dose coronary CTA (Group A, n = 82), while keeping the total dose unchanged. Each of the two CTA scans was processed with a different deep-learning reconstruction algorithm. Routine-dose coronary CTA (Group B, n = 86) and routine-dose aortic CTA (Group C, n = 77) with hybrid iterative reconstruction were used as reference for evaluating the acceptability for surgical planning (A vs. B for aortic valve; A vs. C for access route) and for comparing both the diagnostic and objective image quality (A vs. B for coronary arteries; A vs. C for aortoiliac arteries).
Results: The mean effective dose in Group A was 8.22 ± 0.83 mSv, representing a 57% reduction of the routine-dose TAVI planning CT, that is, a routine-dose coronary CTA plus a routine-dose aortic CTA on the same scanner model. With respect to B and C, images in A were scored higher for evaluating the aortic valve (p = 0.045) and the access route (p = 0.014) and for diagnosing the thoracic aorta and iliac segments (p < 0.050), while the diagnostic confidence were comparable on the coronary arteries (p > 0.050), abdominal aorta (p = 0.276), and femoral segment (p = 0.816). The image noise in A was found to be 21%-55% lower, leading to a significant increase in contrast-to-noise ratio (CNR) by 63%-114% (p < 0.050).
Conclusion: Reduced-dose TAVI planning CT is feasible on 8-cm detector scanners by using deep-learning reconstruction algorithms, showing promise of implementing the examination in imaging settings that are more commonly accessible.
Keywords: computed tomography angiography; deep learning reconstruction; radiation dose; transcatheter aortic valve implantation.
© 2025 The Author(s). Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
Two of the authors (J.L. and G.Z.) are scientific researchers with the United Imaging Healthcare. The remaining authors declare no relationships with any companies.
Figures



References
-
- Cahill TJ, Chen M, Hayashida K, et al. Transcatheter aortic valve implantation: current status and future perspectives. Eur Heart J. 2018;39(28):2625‐2634. - PubMed
-
- Leon MB, Smith CR, Mack MJ, et al. Transcatheter or surgical aortic‐valve replacement in intermediate‐risk patients. N Engl J Med. 2016;374(17):1609‐1620. - PubMed
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic‐valve replacement in high‐risk patients. N Engl J Med. 2011;364(23):2187‐2198. - PubMed
-
- Mack MJ, Leon MB, Thourani VH, et al. Transcatheter aortic‐valve replacement with a balloon‐expandable valve in low‐risk patients. N Engl J Med. 2019;380(18):1695‐1705. - PubMed
-
- Blanke P, Schoepf UJ, Leipsic JA. CT in transcatheter aortic valve replacement. Radiology. 2013;269(3):650‐669. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
