

Stem cell therapy for erectile dysfunction: promise or reality? - a systematic review and meta-analysis of clinical trials
- PMID: 40883730
- PMCID: PMC12395856
- DOI: 10.1186/s12894-025-01913-5
Stem cell therapy for erectile dysfunction: promise or reality? - a systematic review and meta-analysis of clinical trials
Abstract
Background: The outcomes of clinical trials on stem cell therapy (SCT) on erectile dysfunction (ED) treatment are promising but there is still no conclusive evidence regarding its efficacy. The aim of this meta-analysis is to compile studies that assess the effectiveness of SCT on ED to reach a more reliable conclusion.
Methods: The meta-analysis was registered to PROSPERO (CRD42024540511). We utilized the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline to report the outcomes. Articles published from January 2000 to May 2024 were included for systematic review. We performed a systematic search using keywords: "stem cell" AND ("erectile dysfunction" OR "erectile function" OR "erection" OR "impotence").
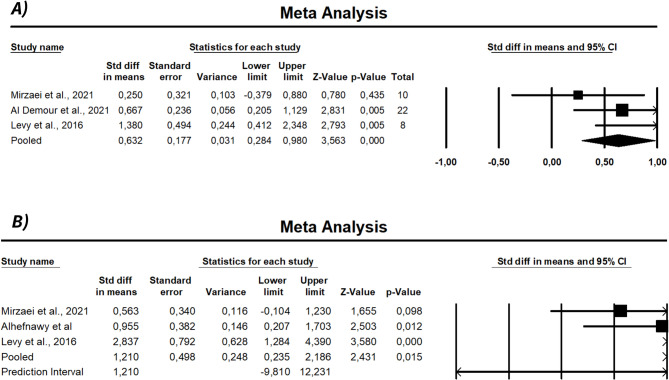
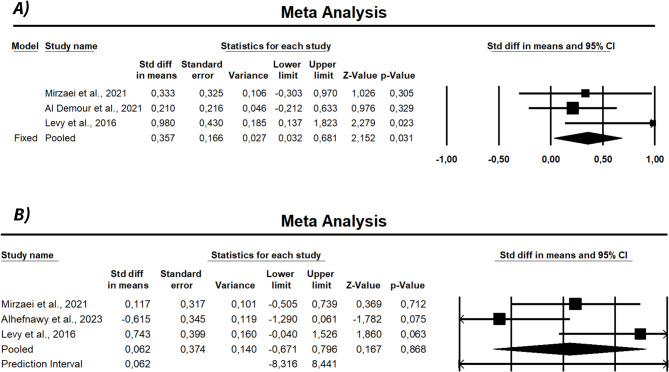
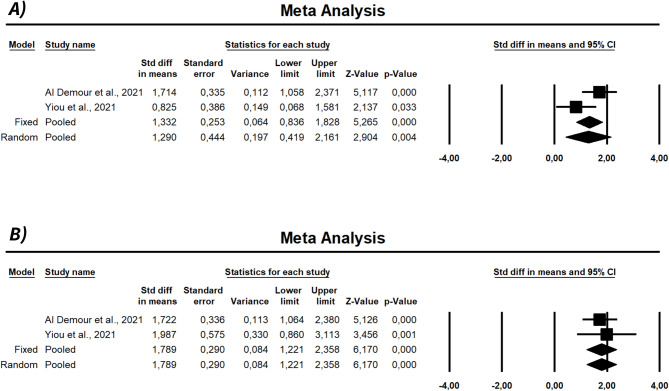
Results: We initially identified 2,013 studies in full publications or abstracts using the search terms. Eleven studies were included in systematic review and six of them were included in meta-analysis. Most studies included in systematic review reported improvements in erectile function following intracavernosal SCT. The meta-analysis revealed significant improvements at six months in international index of erectile function-5 (IIEF-5), international index of erectile function-erectile function domain) IIEF-EF, erectile hardness score (EHS), and peak systolic velocity (PSV) (p < 0.05). End-diastolic velocity (EDV) increased significantly at 3 months (p = 0.031) but not at six months (p = 0.868). Heterogeneity ranged from low to high (I² = 0-71.2%). No significant publication bias was detected (Egger's test p > 0.05).
Conclusion: Intracavernosal SCT may increase scores on the questionnaires evaluated compared to baseline at six months which currently represent the longest reported follow-up duration but comparative trials with longer follow-up periods are needed to draw more definitive conclusions and reveal long-term effect.
Keywords: ED; Erectile dysfunction; Regenerative therapy; Stem cell.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Gratzke C, Angulo J, Chitaley K, et al. Anatomy, physiology, and pathophysiology of erectile dysfunction. J Sex Med. 2010;7(3):445–7. - PubMed
-
- NIH Consensus Conference. Impotence. JAMA. 1993;270:83. - PubMed
-
- Fisher WA, Eardley I, McCabe M, Sand M. Erectile dysfunction (ED) is a shared sexual concern of couples I: couple conceptions of ED. J Sex Med. 2009;6(10):2746–60. - PubMed
-
- Al Demour S, Adwan S, Jafar H, Rahmeh R, Alhawari H, Awidi A. Safety and efficacy of 2 intracavernous injections of allogeneic wharton’s jelly-derived mesenchymal stem cells in diabetic patients with erectile dysfunction: phase 1/2 clinical trial. Urol Int. 2021;105(11–12):935–43. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
