

Clinical-transcriptomic classification of lumbar disc degeneration enhanced by machine learning
- PMID: 40883814
- PMCID: PMC12395706
- DOI: 10.1186/s40779-025-00637-9
Clinical-transcriptomic classification of lumbar disc degeneration enhanced by machine learning
Abstract
Background: Lumbar disc degeneration (LDD) displays considerable heterogeneity in terms of clinical features and pathological changes. However, researchers have not clearly determined whether the transcriptome variations in LDD could be used to identify or interpret the causes of heterogeneity in clinical features. This study aimed to identify the transcriptomic classification of degenerated discs in LDD patients and whether the molecular subtypes of LDD could be accurately predicted using clinical features.
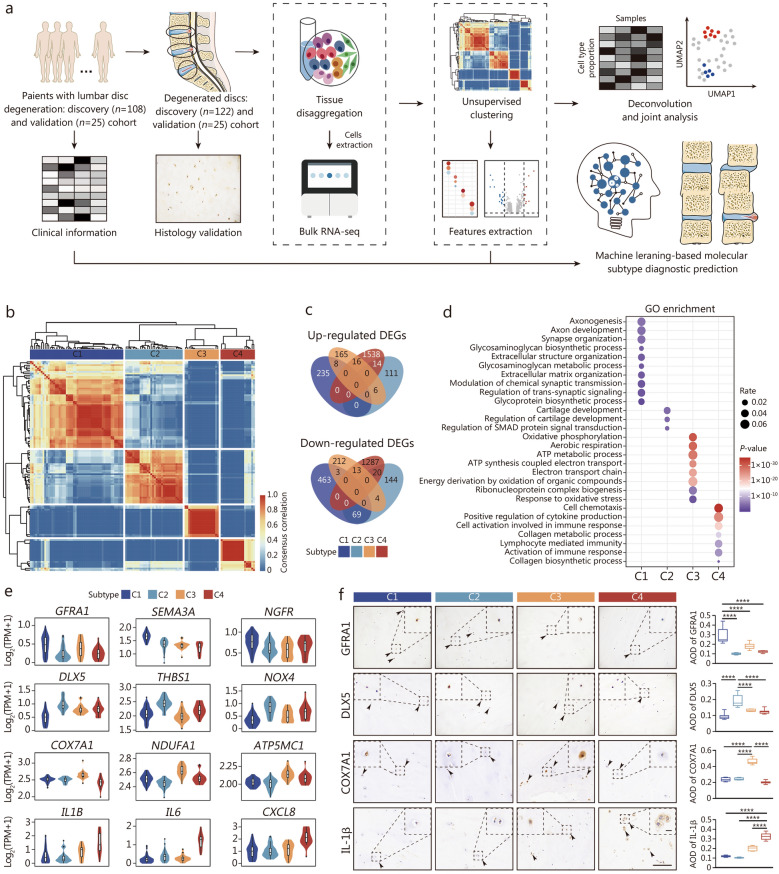
Methods: One hundred and twenty-two nucleus pulposus (NP) tissues from 108 patients were consecutively collected for bulk RNA sequencing (RNA-seq). An unsupervised clustering method was employed to analyze the bulk RNA matrix. Differential analysis was performed to characterize the transcriptional signatures and subtype-specific extracellular matrix (ECM) dysregulation. The cell subpopulation states of each subtype were inferred by integrating bulk and single-cell sequencing datasets. Transwell and dual-luciferase reporter gene assays were employed to investigate possible molecular mechanisms involved. Machine learning algorithm diagnostic prediction models were developed to correlate molecular classification with clinical features.
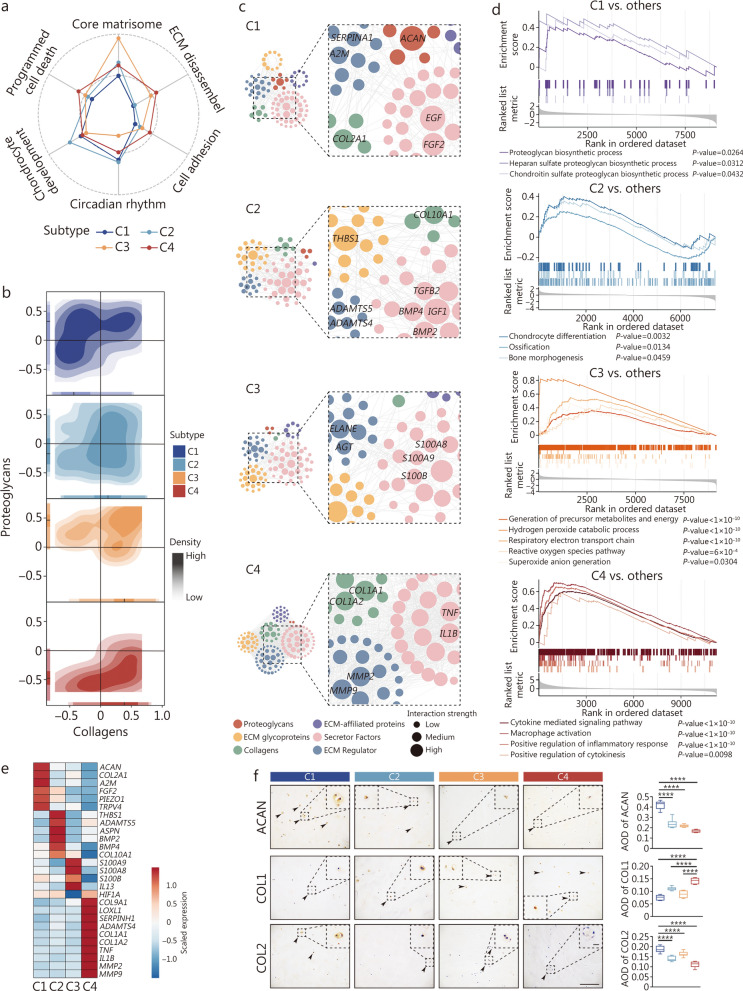
Results: LDD was classified into 4 subtypes with distinct molecular signatures and ECM remodeling: C1 with collagenesis, C2 with ossification, C3 with low chondrogenesis, and C4 with fibrogenesis. Chond1-3 in C1 dominated disc collagenesis via the activation of the mechanosensors TRPV4 and PIEZO1; NP progenitor cells in C2 exhibited chondrogenic and osteogenic phenotypes; Chond1 in C3 was linked to a disrupted hypoxic microenvironment leading to reduced chondrogenesis; Macrophages in C4 played a crucial role in disc fibrogenesis via the secretion of tumor necrosis factor-α (TNF-α). Furthermore, the random forest diagnostic prediction model was proven to have a robust performance [area under the receiver operating characteristic (ROC) curve: 0.9312; accuracy: 0.84] in stratifying the molecular subtypes of LDD based on 12 clinical features.
Conclusions: Our study delineates 4 distinct molecular subtypes of LDD that can be accurately stratified on the basis of clinical features. The identification of these subtypes would facilitate precise diagnostics and guide the development of personalized treatment strategies for LDD.
Keywords: Diagnosis; Lumbar disc degeneration (LDD); Machine learning; Molecular classification; RNA sequencing (RNA-seq); Transcriptome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in accordance to the Declaration of Helsinki and was approved by the Ethics Committee of the Army Medical Center of PLA (2022-312). The information of all patients was deidentified to protect patient privacy. Written informed consent for this study was obtained from all participants. This study was registered in the Chinese Clinical Trial Registry at https://www.chictr.org.cn (ChiCTR2200066854). Consent for publication: Not applicable. Competing interests: All the authors declare that they have no competing interests and that no generative AI or AI-assisted technology was employed in the writing process. The Army Medical Center of PLA supported this submission.
Figures



References
-
- Battié MC, Videman T. Lumbar disc degeneration: epidemiology and genetics. J Bone Joint Surg Am. 2006;88(Suppl 2):3–9. - PubMed
-
- Deyo RA, Mirza SK. Clinical practice herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763–72. - PubMed
-
- Schneiderman G, Flannigan B, Kingston S, Thomas J, Dillin WH, Watkins RG. Magnetic resonance imaging in the diagnosis of disc degeneration: correlation with discography. Spine. 1987;12(3):276–81. - PubMed
-
- Thompson JP, Pearce RH, Schechter MT, Adams ME, Tsang IK, Bishop PB. Preliminary evaluation of a scheme for grading the gross morphology of the human intervertebral disc. Spine. 1990;15(5):411–5. - PubMed
MeSH terms
Grants and funding
- 32270887/National Natural Science Foundation of China
- 82272507/National Natural Science Foundation of China
- 32200654/National Natural Science Foundation of China
- 82430079/National Natural Science Foundation of China
- 82472519/National Natural Science Foundation of China
- 2022YFA1103202/National Key Research and Development Program of China
- CSTB2023NSCQ‑ZDJO008/Natural Science Foundation of Chongqing
- BX20220397/Postdoctoral Innovative Talent Support Program
- SFLKF202201/State Key Laboratory of Trauma, Burns and Combined Injury
- 2023XJS39/Project for Enhancing Innovation of Army Medical University
- ZXZYTSYS09/Talent Innovation Training Program at the Army Medical Center
LinkOut - more resources
Full Text Sources
Miscellaneous
