

Impact of empirical treatment failure on health care resource utilization and costs among female patients with uncomplicated urinary tract infections in a US-based Integrated Health Delivery Network
- PMID: 40884226
- PMCID: PMC12397980
- DOI: 10.18553/jmcp.2025.31.9.879
Impact of empirical treatment failure on health care resource utilization and costs among female patients with uncomplicated urinary tract infections in a US-based Integrated Health Delivery Network
Abstract
Background: Uncomplicated urinary tract infections (uUTIs) are one of the most common outpatient infections in the United States. Despite this, there are limited data on the impact of oral antibiotic treatment failure (TF) on health care resource utilization (HCRU) and costs for patients with empirically treated uUTIs.
Objective: To describe all-cause total health care costs in female patients with uUTIs who fail (TF cohort) and who do not fail (no-TF cohort) initial, empirically prescribed, oral antibiotic treatment. Secondary objectives were to describe all-cause HCRU and UTI-related HCRU and costs in the TF cohort and no-TF cohort.
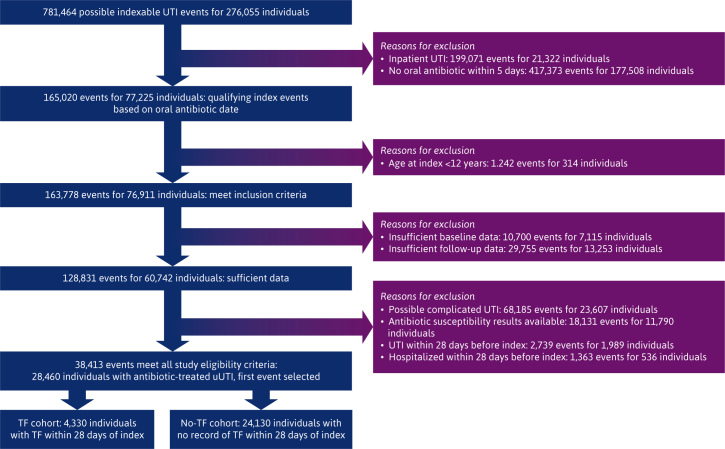
Methods: This study used deidentified electronic health record (EHR) data for female patients aged 12 years and older collected from a US Integrated Delivery Network between January 2016 and January 2023. Eligibility criteria included a uUTI outpatient diagnosis, empirical antibiotic prescription within ±5 days of index uUTI diagnosis, and 12 months or more of EHR activity pre-index and post-index. TF was defined as at least 1 of the following within 28 days after the index date (date of first antibiotic treatment within 5 days of first uUTI diagnosis): second oral antibiotic prescription; intravenous antibiotic administration; or emergency department (ED) or inpatient stay with UTI listed as the primary diagnosis (index uUTI excluded). HCRU and costs 12 months post-index were captured by setting of care, with medical and pharmacy cost estimates based on the most recent available Centers for Medicare and Medicaid Services fee schedule reimbursement rates and prescription costs. Propensity score matching (1:1) was used to control for cohort imbalances.
Results: Of 28,460 patients with a uUTI diagnosis, 4,330 (15.2%) experienced empirical antibiotic TF. Mean age of matched TF and no-TF patients (3,957 per cohort) was 53 years; 95% and 96%, respectively, were White. During the index uUTI episode, the TF cohort had higher mean total all-cause costs ($1,369 vs $482; P < 0.001) and UTI-related costs ($392 vs $78; P < 0.001) and a higher proportion of the TF cohort compared with the no-TF cohort had all-cause inpatient stays (3.1% vs 0.5%; P < 0.001) and ED visits (19.1% vs 7.6%; P < 0.001). All-cause and UTI-related total costs remained significantly higher in the TF cohort across time intervals during the 12-month post-index period, including the 181 to 365 days interval.
Conclusions: Empirical antibiotic TF in female patients with uUTIs results in significantly increased HCRU and costs during the uUTI episode and beyond.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
