

Potential role of immune-related LncRNAs in prognosis of hepatocellular carcinoma: an integrative study
- PMID: 40887519
- PMCID: PMC12399479
- DOI: 10.1007/s12672-025-03497-w
Potential role of immune-related LncRNAs in prognosis of hepatocellular carcinoma: an integrative study
Abstract
Background: Hepatocellular carcinoma (HCC) represents a significant global health concern with persistently high incidence and mortality rates. Immune-related long non-coding RNAs (lncRNAs) may play crucial roles in the pathogenesis and progression of HCC, yet their precise mechanisms remain incompletely elucidated.
Objective: This study aims to explore the potential roles of immune-related lncRNAs in HCC patients through systematic biological approaches, integrating clinical data with bioinformatics analysis, and to construct a COX regression model for predicting patient survival.
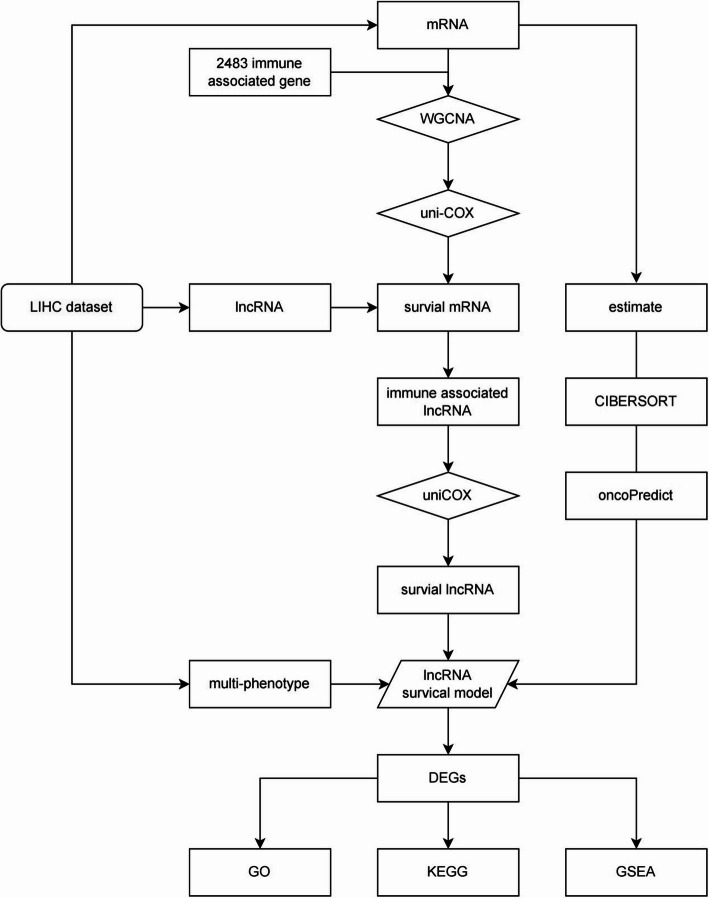
Methods: The HCC dataset from The Cancer Genome Atlas (TCGA) was utilized as the study cohort. Immune-related mRNA and lncRNA data were extracted and screened for their association with HCC patient survival using Weighted Gene Co-expression Network Analysis (WGCNA) algorithm and COX regression method. A COX regression model was subsequently established and validated.
Results: Our investigation revealed that a COX regression model comprising a group of immune-related lncRNAs and mRNAs could accurately predict patient survival in HCC. Specific analyses indicated the pivotal roles of these RNAs in the occurrence and progression of HCC, particularly in immune regulation.
Conclusions: The findings of this study underscore the critical role of immune-related lncRNAs and mRNAs in the prognosis of HCC patients, suggesting their potential as prognostic factors. This discovery provides important insights into the immune modulation mechanisms of HCC, offering novel avenues and methods for personalized therapy and prognostic assessment of HCC.
Keywords: Bioinformatics analysis; Cox regression model; Drug sensitivity; Hepatocellular carcinoma (liver cancer HCC); Immune microenvironment; Immune regulation; Immunotherapy; Long non-coding RNA (lncRNA); Survival prognosis; TCGA database (LIHC).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study used publicly available data and did not involve human participants. Therefore, ethical approval and consent to participate were not required. Consent for publication: All authors have given their consent to publish the results of this study. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
Anoikis-related lncRNA signature predicts prognosis and is associated with immune infiltration in hepatocellular carcinoma.Anticancer Drugs. 2024 Jun 1;35(5):466-480. doi: 10.1097/CAD.0000000000001589. Epub 2024 Mar 11. Anticancer Drugs. 2024. PMID: 38507233
-
The construction and evaluation of a prognostic risk score model for HCC based on MPT-related lncRNAs.Front Oncol. 2025 Jul 28;15:1590094. doi: 10.3389/fonc.2025.1590094. eCollection 2025. Front Oncol. 2025. PMID: 40792280 Free PMC article.
-
A novel prognostic model based on immunogenic cell death-related genes for improved risk stratification in hepatocellular carcinoma patients.J Cancer Res Clin Oncol. 2023 Sep;149(12):10255-10267. doi: 10.1007/s00432-023-04950-5. Epub 2023 Jun 3. J Cancer Res Clin Oncol. 2023. PMID: 37269346 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Long non-coding RNA-based single and combination independent prognostic biomarkers for hepatocellular carcinoma.Discov Oncol. 2025 Sep 2;16(1):1674. doi: 10.1007/s12672-025-03309-1. Discov Oncol. 2025. PMID: 40892177 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources