

Coronary flow reserve increase after 4-year dapagliflozin treatment in patients with type 2 diabetes: the DAPAHEART follow-up study
- PMID: 40887630
- PMCID: PMC12400749
- DOI: 10.1186/s12933-025-02912-4
Coronary flow reserve increase after 4-year dapagliflozin treatment in patients with type 2 diabetes: the DAPAHEART follow-up study
Abstract
Background: Cardiovascular (CV) outcome trials have shown that sodium-glucose cotransporter-2 inhibitors (SGLT2i) reduce CV mortality in type 2 diabetes (T2DM). We previously found that 4 weeks of SGLT2i treatment increased coronary flow reserve (CFR) by 30% and reduced epicardial adipose tissue (EAT) thickness by 19% in T2DM patients with stable coronary artery disease (CAD). However, long-term effects remain unclear. This pilot study aimed to assess the long-term impact of dapagliflozin on CFR and EAT thickness in T2DM patients with CAD.
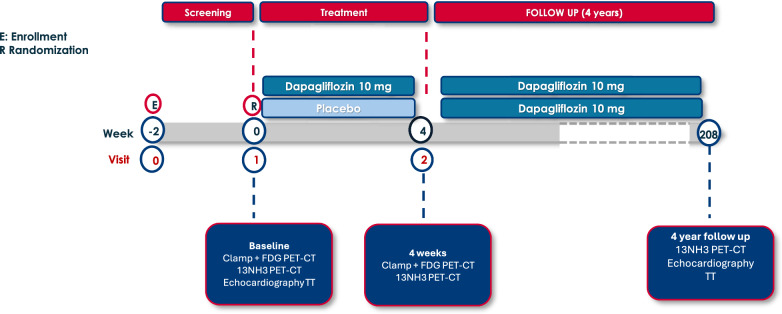
Methods: Patients with T2DM and stable CAD were enrolled in the DAPAHEART trial, a single-center, 4-week, randomized (1:1 dapagliflozin 10 mg vs. placebo), double-blind, controlled study. At the end of the trial, placebo group patients also transitioned to dapagliflozin. CFR and EAT thickness were measured at baseline, after 4 weeks, and after 4 years using 13N-ammonia PET/CT.
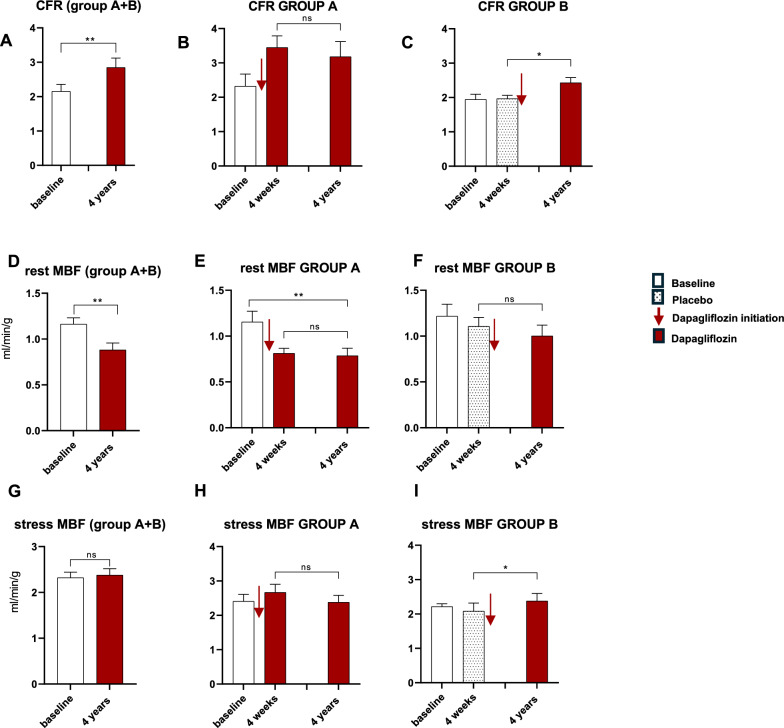
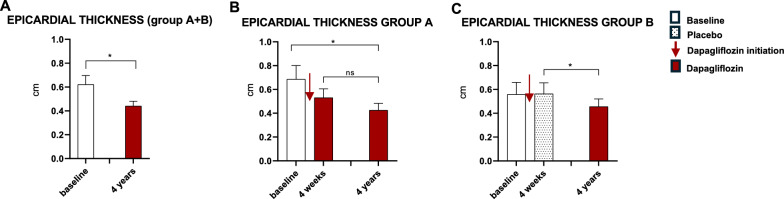
Results: CFR increased 34.4% after 4 years (from 2.15 ± 0.19 at baseline to 2.85 ± 0.26, p = 0.001) with 29.18% reduction in EAT thickness (p = 0.03). BMI decreased in all patients (p = 0.001), but changes in BMI and EAT thickness were not significantly correlated (R2 = 0.0662; p = 0.5), suggesting a weight-independent effect of dapagliflozin on EAT.
Conclusion: The 30% CFR improvement seen after 4 weeks of dapagliflozin persisted at 4 years, together with a significant reduction in EAT thickness, possibly explaining CFR improvement. Similar results in the placebo group after treatment strongly support a causal relationship and underscore the long-term CV benefits of dapagliflozin and its role in reducing CV risk in T2DM patients.
Keywords: Coronary artery disease; Coronary flow reserve; Dapagliflozin; Epicardial adipose tissue; Long-term coronary flow reserve; SGLT2i; Type 2 diabetes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the local ethics committee (Fondazione Policlinico Universitario Agostino Gemelli IRCCS, study protocol code GIA-DAP-16–005) and registered at eudract.ema.europa.eu (EudraCT No. 2016–003614-27) and ClinicalTrials.gov (NCT 03313752). Written informed consent was obtained from all participants. Consent for publication: The corresponding author certifies the accuracy of content, in particular, the names of coauthors and that addresses and affiliations are up to date. The corresponding author certifies that all the co-authors have agreed to all the contents and will notify all the authors when the manuscript is accepted. The corresponding author certifies that all authors have seen and approved the final version of the paper, and all are aware of the submission of the paper. All authors consent to publication. Competing interests: The authors declare no competing interests.
Figures
References
-
- Holman RR, Sourij H, Califf RM. Cardiovascular outcome trials of glucose-lowering drugs or strategies in type 2 diabetes. Lancet. 2014;383:2008–17. 10.1016/S0140-6736(14)60794-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
