

Deep hierarchical subtyping of multi-organ systemic sclerosis trajectories - a EUSTAR study
- PMID: 40890392
- PMCID: PMC12402123
- DOI: 10.1038/s41746-025-01962-y
Deep hierarchical subtyping of multi-organ systemic sclerosis trajectories - a EUSTAR study
Abstract
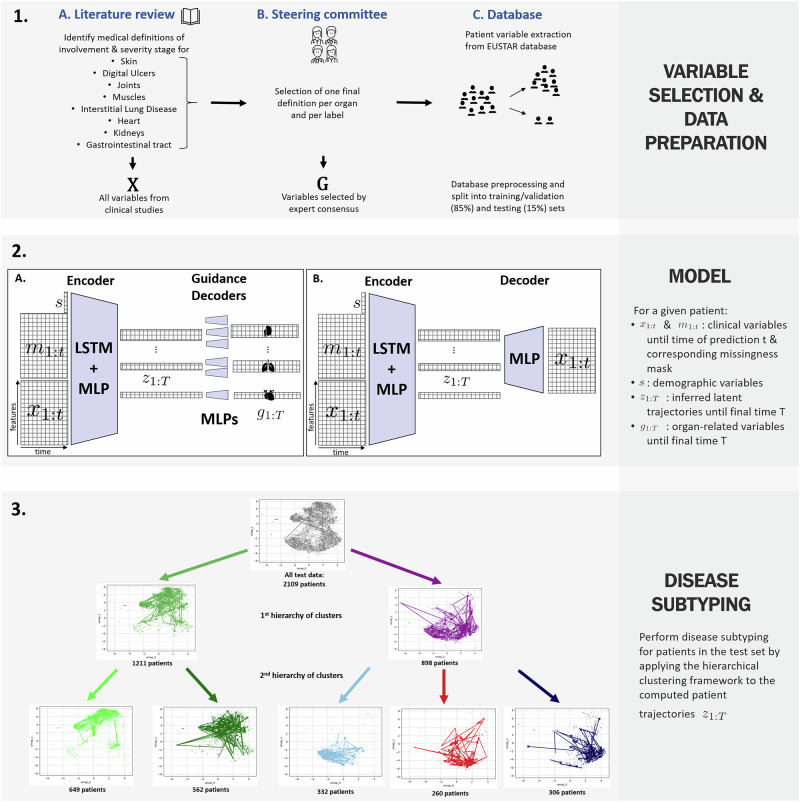
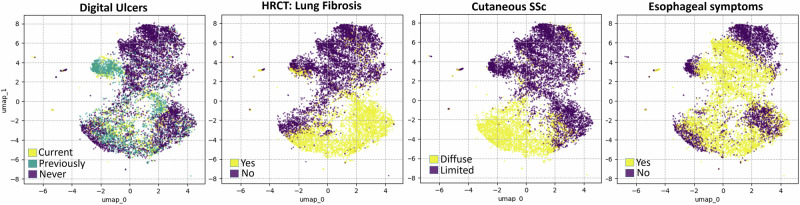
Systemic sclerosis (SSc) is a chronic autoimmune disease with multi-organ involvement. Historically, SSc classification has focused on the type of skin involvement (limited versus diffuse); however, a growing evidence of organ-specific variability suggests the presence of more than two distinct subtypes. We propose a semi-supervised generative deep learning framework leveraging expert-driven definitions of organ-specific involvement and severity. We model SSc disease trajectories in the European Scleroderma Trials and Research (EUSTAR) database, containing 14,000 patients across 67,000 medical visits, and identify clinically meaningful subtypes to enhance patient stratification and prognosis. We systematically evaluate the model's predictive accuracy, robustness to missing data, and clinical interpretability. We identified five patient clusters, separating patients based on the degree of organ involvement. Notably, a subset with limited skin involvement still showed high risks of lung and heart complications, underscoring the importance of data-driven methods and multi-organ models to complement established insights from clinical practice.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.H. has/had consultancy relationship with and/or has received research funding from or has served as a speaker for the following companies in the area of potential treatments for systemic sclerosis and its complications in the last 36 months: Abbvie, Avalyn, CallunaPharma, BMS, Boehringer Ingelheim, Genentech, Janssen, Merck Sharp&Dohme, Medscape, Novartis, Pliant therapeutics, Roche and Werfen. A.H. is a CTD-ILD ERS/EULAR convenor and a EULAR study group leader on the lung in rheumatic and musculoskeletal diseases.OD has/had consultancy relationship with and/or has received research funding from or has served as a speaker for the following companies in the area of potential treatments for systemic sclerosis and its complications in the last two years: 4P-Pharma, Abbvie, Acepodia, Aera, AnaMar, Anaveon AG, Argenx, Boehringer Ingelheim, BMS, Calluna, Cantargia AB, Citus AG, CSL Behring, Galderma, Galapagos, Hemetron AG, Innovaderm, Lilly, MSD Merck, Mitsubishi Tanabe; Nkarta Inc., Orion, Pilan, Quell, Scleroderma Research Foundation, EMD Serono, Topadur and UCB. Patent issued “mir-29 for the treatment of systemic sclerosis” (US8247389, EP2331143). OD is a co-founder of CITUS AG. All other authors declare no competing interests.
Figures





References
-
- Denton, C. P. & Khanna, D. Systemic sclerosis. Lancet390, 1685–1699 (2017). - PubMed
-
- Del Galdo, F. et al. Eular recommendations for the treatment of systemic sclerosis: 2023 update. Ann. Rheum. Dis.84, 29–40 (2025). - PubMed
-
- Elhai, M. et al. Stratification in systemic sclerosis according to autoantibody status versus skin involvement: a study of the prospective eustar cohort. Lancet Rheumatol.4, e785–e794 (2022). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
