

Ultrasonography evaluation of the inferior vena cava collapsibility index and the superior vena cava distensibility index for predicting hypotension during general anesthesia in atrial fibrillation patients: a prospective observational study
- PMID: 40890599
- PMCID: PMC12403413
- DOI: 10.1186/s12871-025-03295-5
Ultrasonography evaluation of the inferior vena cava collapsibility index and the superior vena cava distensibility index for predicting hypotension during general anesthesia in atrial fibrillation patients: a prospective observational study
Abstract
Background: Atrial fibrillation (AF) is a prevalent arrhythmia, the ineffective contraction of the atria leads to a decrease in effective cardiac output. AF patients are prone to hypotension during anesthesia, especially in the early stages of general anesthesia. We explored whether the inferior vena cava collapsibility index (IVCCI) or the superior vena cava distensibility index (SVCDI) could predict the occurrence of post-induction hypotension (PIH) and early intraoperative hypotension (eIOH) in AF patients.
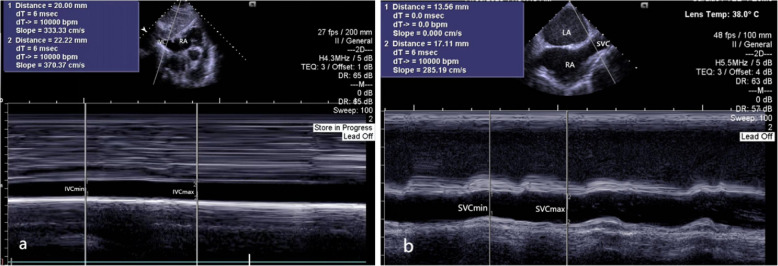
Methods: A total of 77 AF patients undergoing left atrial appendage occlusion under general anesthesia were included in this study. The inferior vena cava was measured before induction and the superior vena cava after induction. The main outcome was the ultrasound measurements of IVCCI and SVCDI in AF patients and their association with hypotension during general anesthesia. Hypotension was classified as the mean arterial pressure (MAP) below 60 mmHg or more than 20% below the baseline level. The correlation between IVCCI, SVCDI and the percentage decrease in MAP was assessed. Receiver operating characteristic (ROC) curves of IVCCI, SVCDI were separately generated to predict PIH and eIOH. Logistic regression was employed to validate the risk factors for PIH and eIOH in AF patients.
Results: AF patients who developed PIH had a significantly higher IVCCI (P < 0.001) and developed eIOH had a significantly higher SVCDI (P < 0.001). ROC curve analysis showed that IVCCI had an accuracy of 85% to predict PIH at a cut-off point more than 34.1% (P < 0.001). SVCDI had an accuracy of 86% to predict eIOH at a cut-off point more than 17.8% (P < 0.001). After adjusting for confounding variables, IVCCI was an independent predictor of PIH (P < 0.001), while SVCDI was an independent predictor of eIOH (P < 0.001).
Conclusion: Preoperative IVCCI > 34.1% indicates a non-invasive predictor of PIH in AF patients; SVCDI > 17.8% suggest a reliable predictor of eIOH in AF patients.
Trial registration: This trial was registered on June 27, 2023 at the China Clinical Trial Center (http://www.chictr.org.cn; No. ChiCTR2300072846).
Keywords: Atrial fibrillation; Early intraoperative hypotension; IVC-CI; Post-induction hypotension; SVC-DI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Institutional Ethics Committee of Shanghai Zhoupu Hospital (Ethical number: 2022-C-027-E0) and registered in Chinese Clinical Trial Register (registration number: ChiCTR2300072846). The study was also conformed to the ethical standards for medical research involving human subjects, as laid out in the 1964 Declaration of Helsinki and its later amendments.Written informed consent was obtained from each participant. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Masoudi FA, Calkins H, Kavinsky CJ, et al. 2015 ACC/HRS/SCAI left atrial appendage occlusion device societal overview. J Am Coll Cardiol. 2015;66:1497–513. - PubMed
-
- van Waes JA, van Klei WA, Wijeysundera DN, et al. Association between intraoperative hypotension and myocardial injury after vascular surgery. Anesthesiology. 2016;124:35–44. - PubMed
-
- Bijker JB, van Klei WA, Vergouwe Y, et al. Intraoperative hypotension and 1-year mortality after noncardiac surgery. Anesthesiology. 2009;111:1217–26. - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology. 2013;119:507–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
