

Fibula single-tunnel versus fibula double-tunnel for both anterior talofibular ligament and calcaneofibular ligament reconstruction: a biomechanical comparison
- PMID: 40890679
- PMCID: PMC12403436
- DOI: 10.1186/s12891-025-08994-1
Fibula single-tunnel versus fibula double-tunnel for both anterior talofibular ligament and calcaneofibular ligament reconstruction: a biomechanical comparison
Abstract
Background: Anatomic ligament repair surgery, despite being a tremendous technical challenge in treating chronic lateral ankle instability patients, remains the gold standard for this condition. The fibula single-tunnel and double-tunnel techniques are effective for intraoperative reconstruction of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL). However, which approach is more appropriate is a subject of debate.
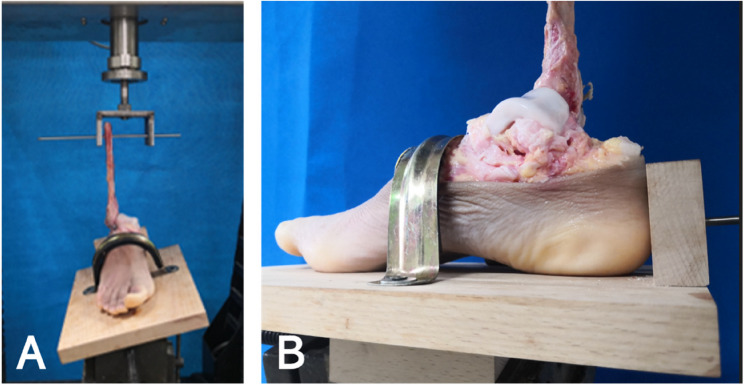
Methods: Twelve fresh frozen cadaveric ankles were randomly divided into 2 groups of 6 specimens: fibula single-tunnel reconstruction group and fibula double-tunnel reconstruction group. The specimens were tested for ankle joint laxity on the plane radiographs with 150 N anterior drawer force and 150 N varus stress force. The anterior talar displacement and talar tilt angle were measured at states of intact, cut and reconstruction of both ATFL and CFL. Then, the reconstructed specimens were loaded to ultimate failure to determine the strength and stiffness of each construct.
Results: There were no significant differences between the two groups in the anterior talar displacement and talar tilt angle at the states of intact, cut and reconstruction of both the ATFL and CFL. There were no significant differences between the two groups in the ultimate load failure and stiffness after reconstruction of both the ATFL and CFL.
Conclusions: In patients undergoing ligament reconstruction surgery for ankle instability, both single-tunnel reconstruction of the fibula and double-tunnel reconstruction of the fibula were able to achieve better results. There was no significant difference between these two surgical procedures in our study. The long-term survival of the ankle joint after both techniques remains to be studied.
Keywords: Anterior talofibular ligament; Biomechanical; Calcaneofibular ligament; Chronic ankle instability; Ligament reconstruction.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for this study was obtained from the institutional review board of the Affiliated Dalian Municipal Friendship Hospital of Dalian Medical University (Approval ID: YY-LL-2022-023). Written informed consent was obtained from donor's next of kin for medical treatment and research. Competing interests: The authors declare no competing interests.
Figures







Similar articles
-
Comparison Between the Simultaneous Reconstructions of the Anterior Talofibular Ligament and Calcaneofibular Ligament and the Single Reconstruction of the Anterior Talofibular Ligament for the Treatment of Chronic Lateral Ankle Instability.J Foot Ankle Surg. 2022 May-Jun;61(3):533-536. doi: 10.1053/j.jfas.2021.01.012. Epub 2021 Oct 22. J Foot Ankle Surg. 2022. PMID: 34785128
-
Biomechanical comparison of reconstruction techniques in simulated lateral ankle ligament injury.Am J Sports Med. 1995 Nov-Dec;23(6):678-82. doi: 10.1177/036354659502300607. Am J Sports Med. 1995. PMID: 8600733
-
A novel 9-region systematic assessment tool for separated ossicle at the fibular tip effects on lateral ankle ligament complex integrity: a cadaveric study.Surg Radiol Anat. 2014 Apr;36(3):281-8. doi: 10.1007/s00276-013-1165-6. Epub 2013 Jul 31. Surg Radiol Anat. 2014. PMID: 23900504
-
Anatomy of anterior talofibular ligament and calcaneofibular ligament for minimally invasive surgery: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2017 Jun;25(6):1892-1902. doi: 10.1007/s00167-016-4194-y. Epub 2016 Jun 13. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27295109
-
Anterior lateral ankle ligament damage and anterior talocrural-joint laxity: an overview of the in vitro reports in literature.Clin Biomech (Bristol). 2001 Oct;16(8):635-43. doi: 10.1016/s0268-0033(01)00054-7. Clin Biomech (Bristol). 2001. PMID: 11535344
References
-
- Sammarco VJ. Complications of lateral ankle ligament reconstruction. Clin Orthop Relat Res. 2001;391:123–32. - PubMed
-
- Fujii T, Kitaoka HB, Watanabe K, Luo ZP, An KN. Comparison of modified Broström and Evans procedures in simulated lateral ankle injury. Med Sci Sports Exerc. 2006;38(6):1025–31. - PubMed
-
- Jung HG, Shin MH, Park JT, Eom JS, Lee DO, Lee SH. Anatomical reconstruction of lateral ankle ligaments using free tendon allografts and Biotenodesis screws. Foot Ankle Int. 2015;36(9):1064–71. - PubMed
-
- Korkala O, Sorvali T, Niskanen R, Haapala J, Tanskanen P, Kuokkanen H. Twenty-year results of the Evans operation for lateral instability of the ankle. Clin Orthop Relat Res. 2002;405:195–8. - PubMed
-
- Krips R, Brandsson S, Swensson C, van Dijk CN, Karlsson J. Anatomical reconstruction and Evans tenodesis of the lateral ligaments of the ankle. Clinical and radiological findings after follow-up for 15 to 30 years. J Bone Joint Surg Br Volume. 2002;84(2):232–6. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
