

Plasma phenylalanine is associated with hospital mortality in acute respiratory distress syndrome: a prospective metabolic profiling cohort study
- PMID: 40890886
- PMCID: PMC12403401
- DOI: 10.1186/s40001-025-03043-y
Plasma phenylalanine is associated with hospital mortality in acute respiratory distress syndrome: a prospective metabolic profiling cohort study
Abstract
Background: Phenylalanine accumulation is associated with inflammation, immune system activation, and oxidative stress-all of which are involved in the pathophysiology of acute respiratory distress syndrome (ARDS). This study evaluated the correlation between longitudinal changes in plasma phenylalanine levels and clinical outcomes in patients with ARDS.
Methods: This prospective observational cohort study conducted in Taiwan focused on plasma amino acid profiling in ARDS patients between February 2017 and June 2018, and again between November 2021 and October 2023. Serial changes in plasma amino acid levels and clinical variables measured at days 1, 3, and 7 after ARDS onset were compared with clinical outcomes.
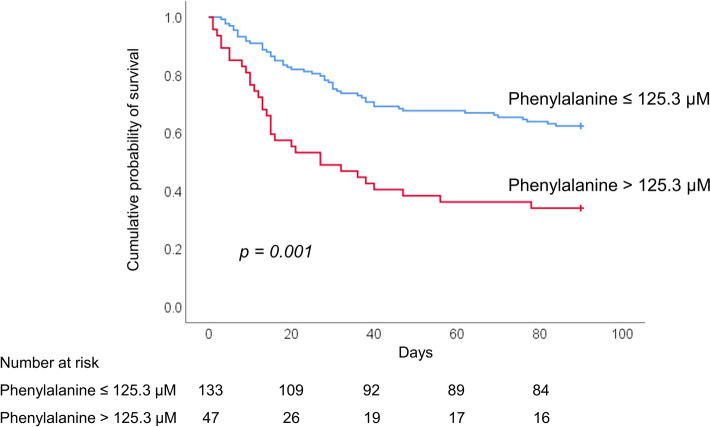
Results: This study included 214 ICU patients, including 180 patients with ARDS and 34 patients without. Among ARDS patients, the in-hospital mortality rate was 45%. Plasma phenylalanine levels were significantly higher among ARDS patients than among ICU controls at all timepoints (days 1, 3, and 7). Plasma phenylalanine levels and phenylalanine/tyrosine ratios were significantly higher among non-survivors than among ARDS survivors throughout the observation period (all p < 0.05). ARDS patients with high plasma phenylalanine levels (> 125.3 µM; 47 patients; 26.1%) presented a significantly elevated risk of organ failure (i.e., higher APACHE II and SOFA scores) as well as 28-, 60-, 90-day, and all-cause hospital mortality, compared to those with low plasma phenylalanine levels (≤ 125.3 µM; 133 patients; 73.9%) (all p < 0.05). Multivariable logistic regression analysis revealed that plasma phenylalanine levels and phenylalanine/tyrosine ratios at day 1 were independently associated with hospital mortality (adjusted OR 1.009, [95% CI 1.001-1.017], p = 0.037 and adjusted OR 2.851, [95% CI 1.045-7.780], p = 0.041, respectively). A plasma phenylalanine level of > 125.3 µM had the highest predictive value for in-hospital mortality (adjusted OR 4.825, [95% CI 1.324-17.583], p = 0.017).
Conclusions: Plasma phenylalanine at the onset of ARDS is independently associated with hospital mortality. These findings indicate that phenylalanine metabolism may be disrupted early in the course of ARDS. They also indicate that plasma phenylalanine levels could serve as an early prognostic metabolic biomarker and potential therapeutic target.
Keywords: Acute respiratory distress syndrome; Metabolomics; Mortality; Outcomes; Oxidative stress; Phenylalanine; Tyrosine.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki after receiving approval from the Institutional Review Board for Human Research of Chang Gung Memorial Hospital (CGMH IRB No. 201407524B0, 201801052A3, 201801497B0, 202100595A3, 202201833A3, and 202300897A3), and informed consent from all subjects involved in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Bos LDJ, Ware LB. Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes. Lancet. 2022;400(10358):1145–56. - PubMed
-
- Gorman EA, O’Kane CM, McAuley DF. Acute respiratory distress syndrome in adults: diagnosis, outcomes, long-term sequelae, and management. Lancet. 2022;400(10358):1157–70. - PubMed
-
- Wishart DS. Metabolomics for investigating physiological and pathophysiological processes. Physiol Rev. 2019;99(4):1819–75. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
