

Minimally Invasive Surgery vs Medical Management Alone for Intracerebral Hemorrhage: The MIND Randomized Clinical Trial
- PMID: 40892424
- PMCID: PMC12406146
- DOI: 10.1001/jamaneurol.2025.3151
Minimally Invasive Surgery vs Medical Management Alone for Intracerebral Hemorrhage: The MIND Randomized Clinical Trial
Abstract
Importance: It remains uncertain whether surgical evacuation improves functional outcomes in patients with supratentorial intracerebral hemorrhage (ICH).
Objective: To compare the safety and efficacy of minimally invasive surgery with the Artemis Neuro Evacuation Device to guideline-based medical management alone for spontaneous supratentorial ICH.
Design, setting, and participants: The MIND open-label, multicenter randomized clinical trial randomized patients with spontaneous supratentorial ICH in a 2:1 ratio to either minimally invasive surgery or medical management alone. Participants were enrolled at 32 participating global sites between February 6, 2018, and August 28, 2023. This article reports on the primary trial outcome. Of 4066 eligible adult patients (aged 18-80 years) with moderate- to large-volume supratentorial ICH (20-80 mL), baseline National Institutes of Health Stroke Scale score of 6 or higher, and Glasgow Coma Scale score between 5 and 15, 154 were randomized to minimally invasive surgery and 82 to medical management. Data were analyzed from February to September 2024.
Intervention: Minimally invasive surgery (within 72 hours of symptom onset) plus medical management or medical management alone.
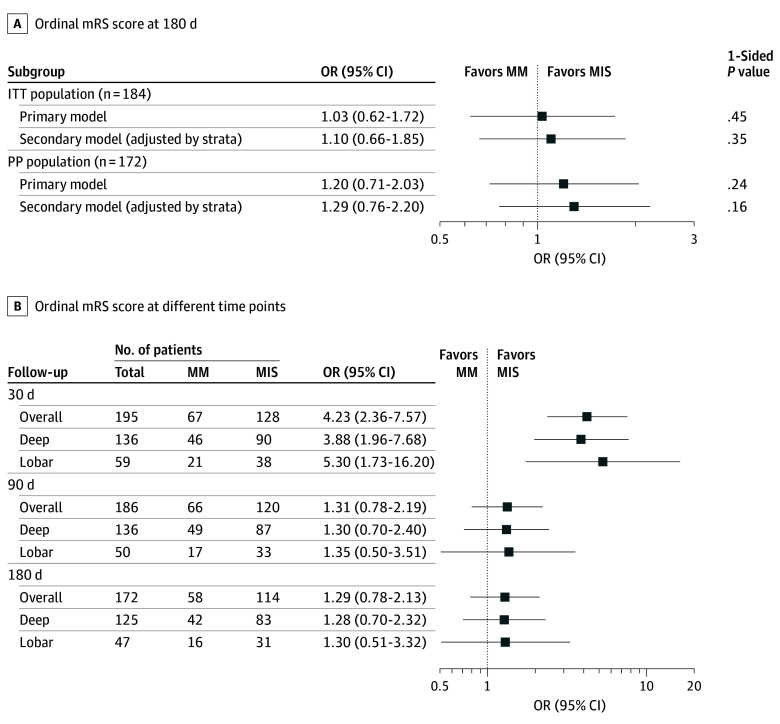
Main outcomes and measures: The primary efficacy outcome was 180-day combined death and disability via ordinal modified Rankin Scale score (range, 0 [no symptoms] to 6 [death]). The primary safety outcome was 30-day mortality.
Results: Following an independent feasibility analysis prompted by the publication of positive results of a contemporaneous ICH trial, enrollment was stopped early at 236 participants. Overall median (IQR) participant age was 60 (50-70) years, 87 participants (36.9%) were female, 164 (69.5%) had primarily deep bleeds, and 72 (30.5%) had primarily lobar bleeds. Efficacy results of the primary model analysis suggested lack of evidence for the superiority of minimally invasive surgery over medical management (odds ratio [OR], 1.03; 96% CI, 0.62-1.72; P = .45). The adjusted model's mean OR was also nonsignificantly greater than 1 (OR, 1.10; 96% CI, 0.66-1.85; P = .35). By 30 days, 11 participants (7.2%) in the surgery group and 8 (9.8%) in the medical management group died (difference, -2.5%; 95% CI, -11.7% to 4.8%).
Conclusions and relevance: In the MIND randomized clinical trial, minimally invasive surgery within 72 hours did not significantly reduce 30-day mortality or improve 180-day disability in patients with supratentorial ICH compared to medical management alone.
Trial registration: ClinicalTrials.gov Identifier: NCT03342664.
Conflict of interest statement
Figures

References
-
- Greenberg SM, Ziai WC, Cordonnier C, et al. ; American Heart Association/American Stroke Association . 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2022;53(7):e282-e361. doi: 10.1161/STR.0000000000000407 - DOI - PubMed
-
- Ziai WC, Badihian S, Ullman N, et al. Hemorrhage expansion rates before and after minimally invasive surgery for intracerebral hemorrhage: post hoc analysis of MISTIE II/III. Stroke Vasc Intervent Neurol. 2024;0(0):e001165. doi: 10.1161/SVIN.123.001165 - DOI
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
