

This is a preprint.
Virtual Coronary Artery Bypass Grafting
- PMID: 40894027
- PMCID: PMC12393576
- DOI: 10.21203/rs.3.rs-7320100/v1
Virtual Coronary Artery Bypass Grafting
Abstract
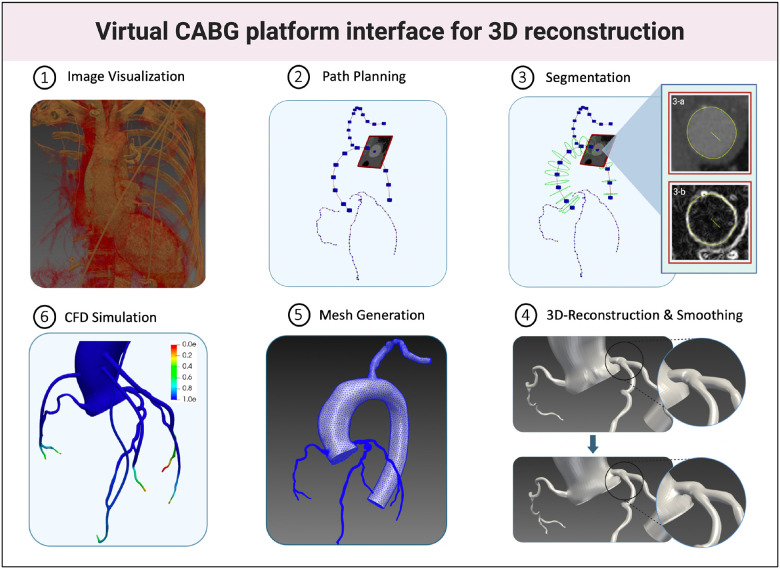
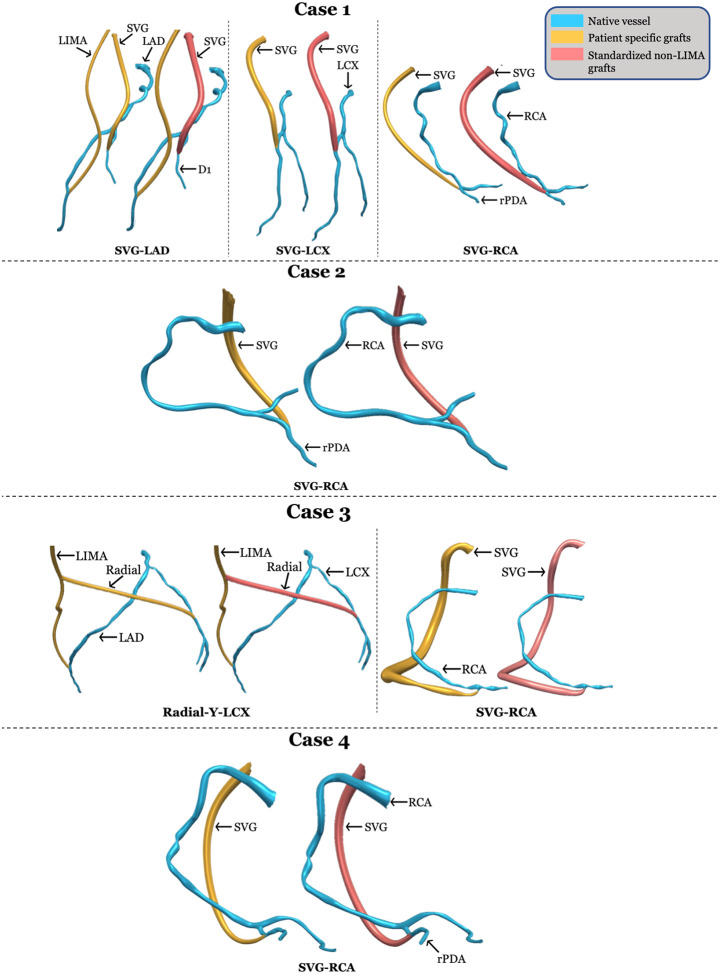
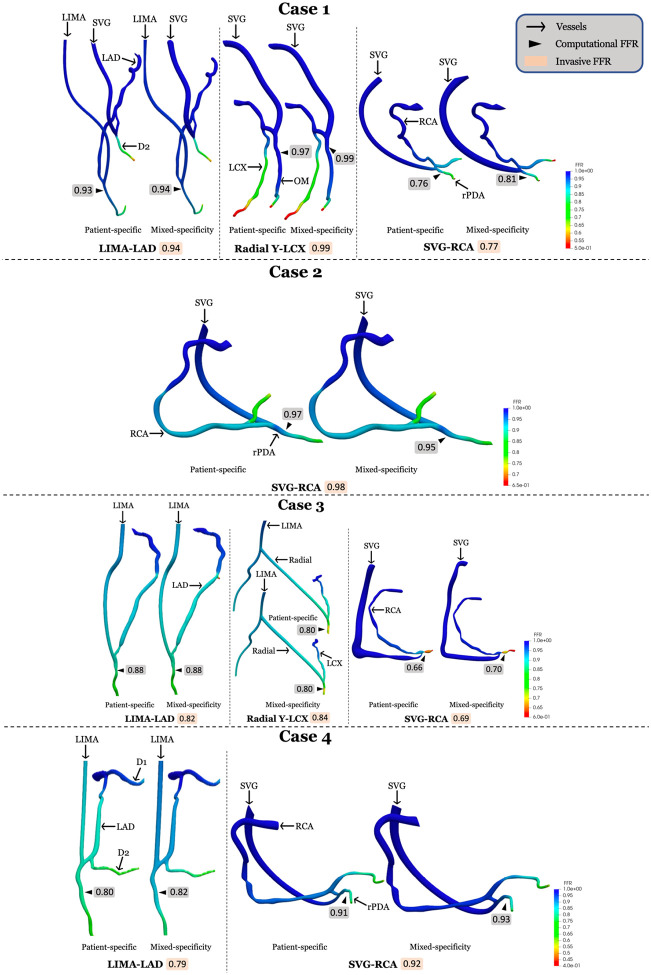
Coronary artery bypass grafting (CABG) offers superior long-term survival over percutaneous coronary intervention (PCI) or medical therapy in patients with complex coronary artery disease (CAD). This prospective proof-of-concept study aims to develop and validate a non-invasive computational platform that integrates coronary computed tomographic angiography (CCTA) and computational fluid dynamics (CFD) to predict post-CABG hemodynamics, including virtual grafting and fractional flow reserve (FFR) estimation. Four patients with stable multi-vessel CAD undergoing elective CABG were included. Pre-CABG CCTA was used for 3D reconstruction of coronary anatomy. Virtual bypass grafting was performed using both patient-specific graft sizes, derived from post-operative imaging and mixed-specificity graft sizes using patient-specific LIMA and standardized non-LIMA graft sizes, derived from population averages. CFD simulations were used to estimate post-CABG FFR and validated against invasive FFR measurements. Computational FFR showed strong correlation with invasive FFR (patient-specific: r2 = 0.92; mixed-specificity: r2 = 0.88). Bland-Altman analysis demonstrated minimal bias (patient-specific: 0.006 ± 0.027; mixed-specificity: -0.007 ± 0.029). Agreement with invasive FFR was 90% for patient-specific grafts (κ = 0.74, p = 0.016) and 80% for mixed-specificity grafts (κ = 0.41, p = 0.107). This virtual CABG model represents a significant advancement over existing non-invasive systems by accurately predicting post-operative hemodynamics and FFR, offering potential to optimize graft strategies and reduce reliance on invasive FFR. Future studies should explore clinical integration and large-scale validation to enhance CABG surgical planning and improve patient outcomes.
Keywords: Computational Fluid Dynamics; Coronary Artery Bypass Grafting; Fractional Flow Reserve; Virtual Grafting.
Conflict of interest statement
Yiannis S. Chatzizisis: Speaker honoraria, advisory board fees, and research grant from Boston Scientific Inc.; Advisory board fees and research grant from Medtronic Inc.; Issued U.S. patent (No. 11,026,749) and international patent pending (application No. PCT/US2020/057304) for the invention entitled “Computational simulation platform for the planning of interventional procedures”; Co-founder of ComKardia Inc.
Figures



References
-
- Doenst T. et al. PCI and CABG for treating stable coronary artery disease: JACC review topic of the week. J Am Coll Cardiol. 73, 964–976 (2019). - PubMed
-
- Lawton J. S. et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization. J Am Coll Cardiol. 79, e21–e129 (2022). - PubMed
-
- Botman C. J. et al. Does stenosis severity of native vessels influence bypass graft patency? A prospective fractional flow reserve–guided study. Ann Thorac Surg. 83, 2093–2097 (2007). - PubMed
-
- Roh J.-H. et al. Fate of grafts bypassing nonischemic versus ischemic inducing coronary stenosis. Am J Cardiol. 122, 1148–1154 (2018). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
