

This is a preprint.
Targeting Plasminogen Activator Inhibitor-1 with a Novel Small Molecule Inhibitor Attenuates Lung Fibrosis
- PMID: 40894033
- PMCID: PMC12393591
- DOI: 10.21203/rs.3.rs-6951289/v1
Targeting Plasminogen Activator Inhibitor-1 with a Novel Small Molecule Inhibitor Attenuates Lung Fibrosis
Abstract
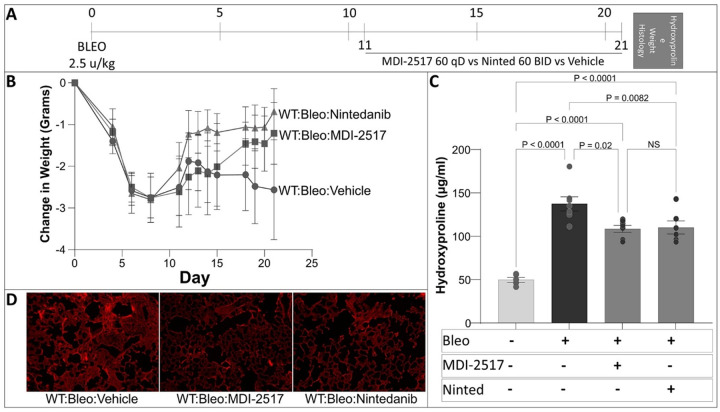
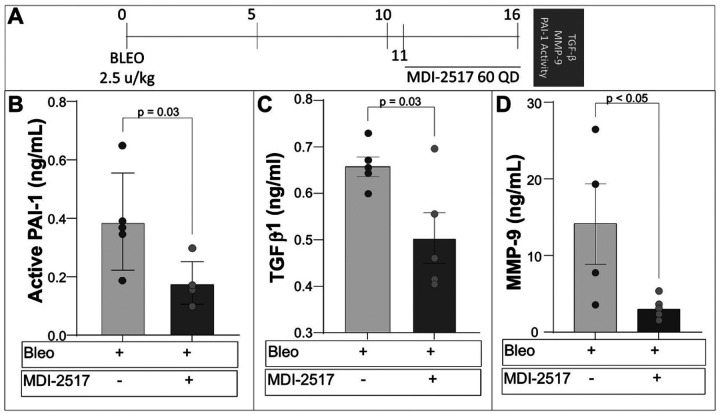
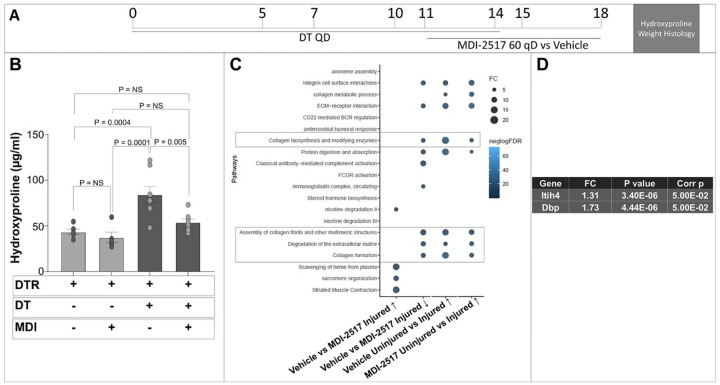
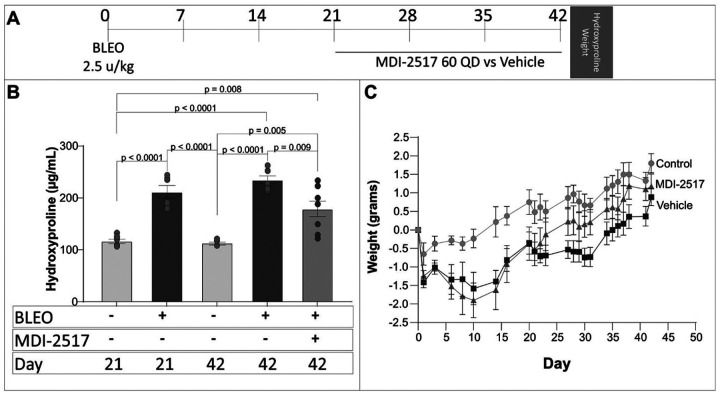
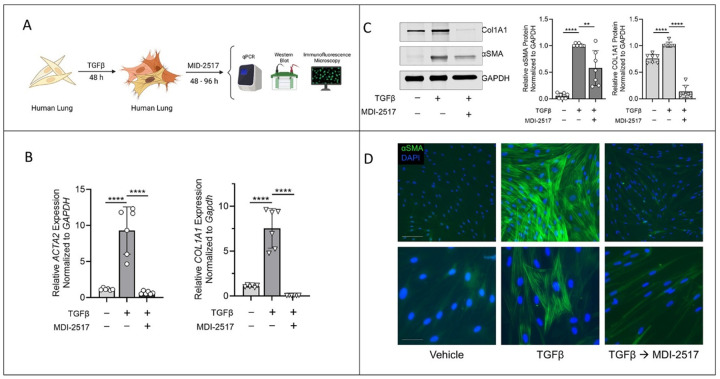
Fibrotic lung diseases are associated with significant morbidity and mortality, and few therapies have been FDA-approved for patients with these conditions. Therefore, developing effective anti-fibrotic treatments represents an unmet clinical need. Plasminogen activator inhibitor 1 (PAI-1) is an attractive therapeutic target as its expression is up-regulated in the context of fibrotic lung disease, and a causal role for PAI-1 in lung fibrogenesis has been established in complementary animal models. Here, we study the efficacy of a novel small molecule PAI-1 inhibitor, MDI-2517, to attenuate lung fibrosis. We observed that MDI-2517 administered during the fibrotic phase of complementary murine models reduces the severity of scarring. Furthermore, we found that MDI-2517 treatment beginning on day 21 after lung injury accelerates fibrosis resolution while in vitro data reveal that this drug reverses myofibroblast differentiation. These results motivate targeting PAI-1 as a therapy for lung fibrosis and highlight MDI-2517 as a promising drug.
Conflict of interest statement
EJS, CDE, and DAL hold interest in MDI Therapeutics which has a license from the University of Michigan for MDI-2517. DAL is a member of the MDI Therapeutics Clinical & Science Advisory Board. DAL, CDE, and MW are inventors on patents for PAI-1 inhibitors. JEG has received research grants from Eli Lilly, Almirall, BMS, Prometheus/Merck, Boehringer Ingelheim, Novartis, Janssen, and AbbVie and has served as an advisor to Eli Lilly, Takeda, BMS, Novartis, Almirall, Janssen, Sanofi, AbbVie, MDI-Therapeutics, and Boehringer Ingelheim. All other authors have declared no conflicts of interest exists.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
