

A Case of Pleomorphic Adenoma of the Submandibular Gland Radiologically Suspected to be Malignant
- PMID: 40895871
- PMCID: PMC12395118
- DOI: 10.7759/cureus.89009
A Case of Pleomorphic Adenoma of the Submandibular Gland Radiologically Suspected to be Malignant
Abstract
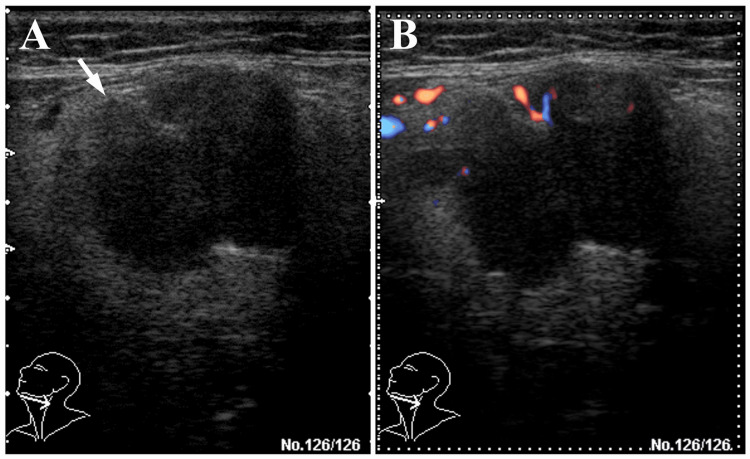
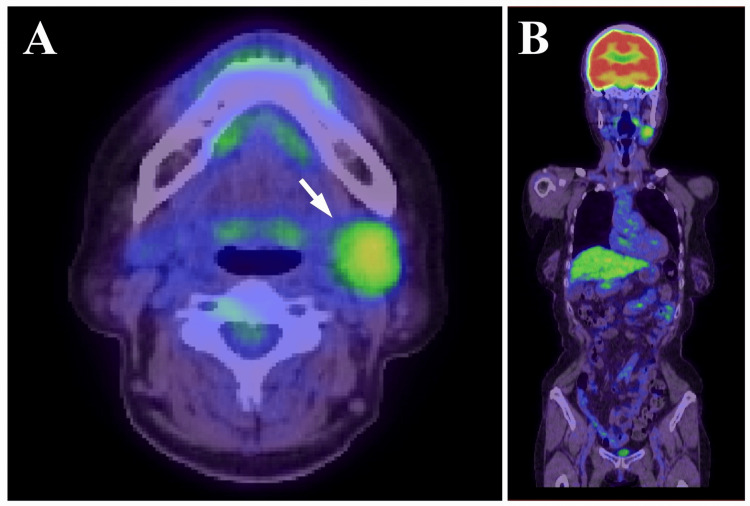
Pleomorphic adenoma (PA) is the most common benign salivary gland tumor, typically arising from the parotid gland. PA of the submandibular gland is relatively uncommon and may present diagnostic challenges, particularly when imaging findings raise suspicion of malignancy. A 66-year-old woman presented with a painless mass in the left submandibular region. Imaging studies including unenhanced computed tomography (CT), magnetic resonance imaging (MRI), ultrasonography (US), and positron emission tomography (PET) revealed a lobulated mass with irregular margins, heterogeneous internal architecture, and partially disrupted capsular structures. PET showed abnormal fluorodeoxyglucose (FDG) accumulation with a maximum standardized uptake value (SUVmax) of 3.70. Based on these findings, malignancies such as adenoid cystic carcinoma or carcinoma ex pleomorphic adenoma (CXPA) were strongly suspected. The tumor was resected under general anesthesia with careful preservation of the capsule and excised en bloc together with the submandibular gland and a portion of the sublingual gland. Histopathological and immunohistochemical analyses revealed no evidence of malignancy, and a final diagnosis of PA was made. This case highlights the diagnostic difficulty of submandibular PA, especially when capsular structures appear ambiguous on imaging. It underscores the limitations of relying solely on imaging modalities and reaffirms the importance of integrating clinical history, imaging, and pathological findings to achieve accurate diagnosis.
Keywords: capsule; differential diagnosis; pleomorphic adenoma; salivary gland tumor; submandibular gland.
Copyright © 2025, Sugino et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





References
-
- Pleomorphic adenoma (benign mixed tumour) of the salivary glands: its diverse clinical, radiological, and histopathological presentation. Lingam RK, Daghir AA, Nigar E, Abbas SA, Kumar M. Br J Oral Maxillofac Surg. 2011;49:14–20. - PubMed
-
- Submandibular gland pleomorphic adenoma: histopathological capsular characteristics and correlation with the surgical outcome. Mantsopoulos K, Goncalves M, Koch M, Iro H, Agaimy A. Ann Diagn Pathol. 2018;34:166–169. - PubMed
-
- Histopathology of parotid pleomorphic adenomas: a “pleomorphic approach” to a demanding lesion. Mantsopoulos K, Thimsen V, Gostian AO, et al. Laryngoscope. 2022;132:73–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials