

A combinatorial oligonucleotide therapy to improve dystrophin restoration and dystrophin-deficient muscle health
- PMID: 40896584
- PMCID: PMC12398789
- DOI: 10.1016/j.omtn.2025.102665
A combinatorial oligonucleotide therapy to improve dystrophin restoration and dystrophin-deficient muscle health
Abstract
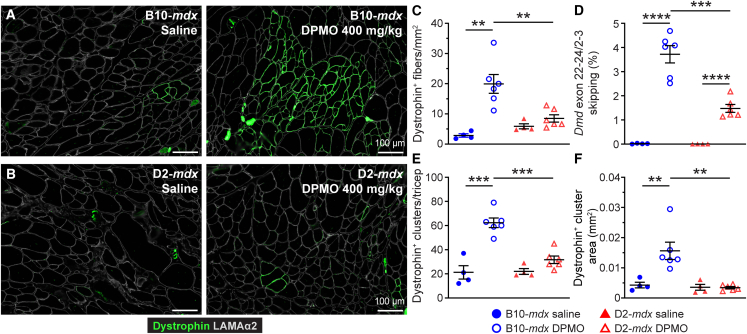
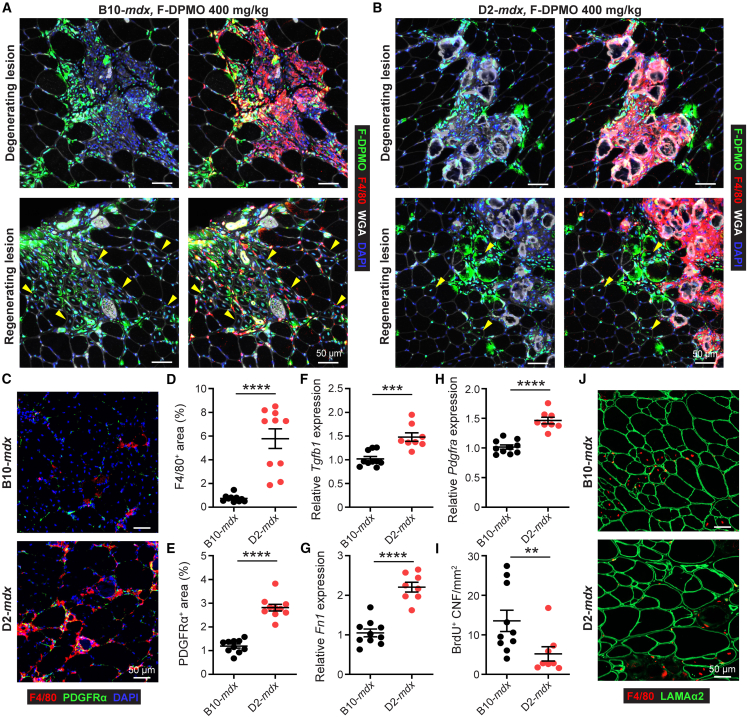
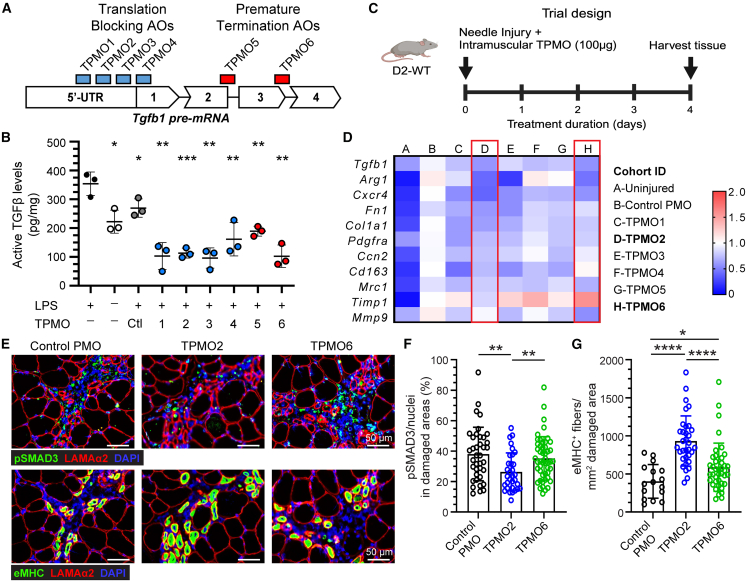
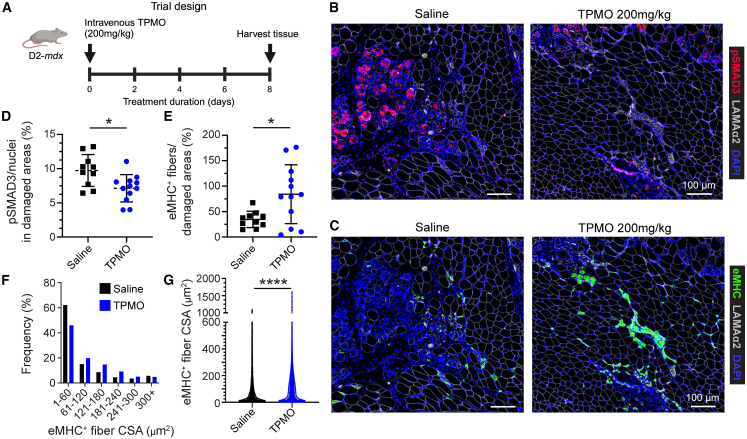
Despite the proven safety of dystrophin-targeting phosphorodiamidate morpholino oligomer (PMO) therapy, poor delivery of the PMOs limit the efficacy of this dystrophin restoring gene therapy for Duchenne muscular dystrophy (DMD). Limited myogenesis and excessive fibrosis in DMD are pathological features that contribute to the poor efficacy of PMOs. We show that the severe DMD mouse model (D2-mdx) not only replicates these pathological features of DMD but also mirrors the resulting PMO-mediated dystrophin restoration deficit. High transforming growth factor β (TGF-β) activity, which is a common feature of DMD patient and D2-mdx muscles, limits myogenesis and causes fibrosis. We developed a TGF-β-targeting PO (TPMO), which when used acutely, lowered macrophage TGF-β activity and signaling in the dystrophic muscle, enhanced muscle regeneration, and enhanced dystrophin restoration when used in combination with dystrophin exon skipping PMO (DPMO). Chronic use of this combination PMO therapy in D2-mdx mice reduced muscle fibrosis and muscle loss, allowed dystrophin restoration in skeletal muscle and heart, and led to an overall enhancement of skeletal muscle function. This approach leverages the safety of PMO-based therapy and represents the first combination PMO treatment for DMD that simultaneously enhances dystrophin restoration, reduces fibrosis, and alleviates myogenic deficits to ultimately improve health and function of dystrophic muscles.
Keywords: Duchenne muscular dystrophy, DMD; MT: Oligonucleotides: Therapies and Applications; PMO; TGF-β; exon skipping; fibroadipogenic; fibrosis; inflammation; muscle regeneration; myogenesis; phosphoro-diamidate morpholino oligomer; transforming growth factor β.
© 2025 The Author(s).
Conflict of interest statement
J.K.J., J.S.N., and Y.J.M. have filed a provisional intellectual property application related to the novel therapeutic strategies disclosed in this manuscript.
Figures




References
LinkOut - more resources
Full Text Sources
