

Factors influencing surgical management and outcomes of colonic trauma: a prospective observational study at three hospitals in Sana'a City, Yemen
- PMID: 40898172
- PMCID: PMC12403608
- DOI: 10.1186/s12893-025-03159-2
Factors influencing surgical management and outcomes of colonic trauma: a prospective observational study at three hospitals in Sana'a City, Yemen
Abstract
Background: Colonic trauma is a major clinical challenge particularly in resource-constrained conflict settings. The optimal surgical management remains debated. This study evaluated the factors influencing the surgical approach and the associated outcomes of colonic trauma in Yemen.
Methods: We conducted a prospective observational cohort study from May 2020 to April 2021, enrolling 90 consecutive patients with traumatic colonic injuries at three hospitals in Sana’a City. We collected data on patient demographics, injury characteristics (including AAST Colon Injury Scale grade), and postoperative outcomes. Statistical analyses were performed to compare patients managed with primary repair and colostomy.
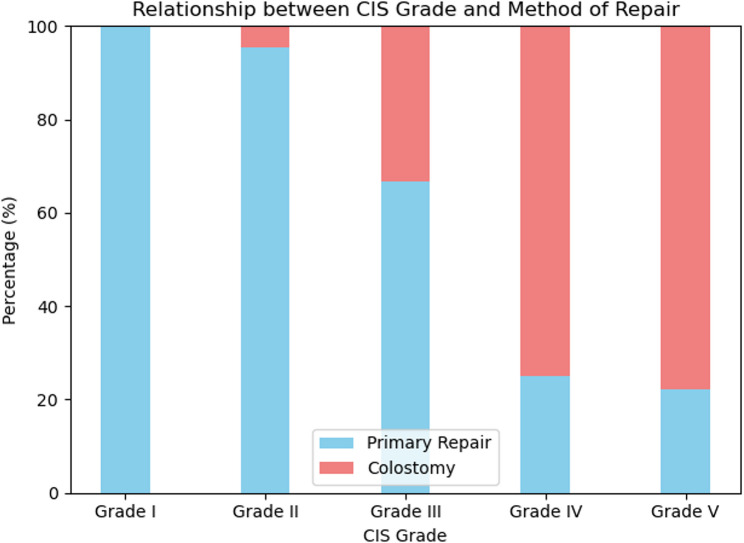
Results: Primary repair was performed in 74 patients (82.2%) and colostomy was performed in 16 patients (17.8%). The decision to perform colostomy was significantly associated with gunshot wounds (P = 0.002), severe fecal contamination (P < 0.001), and high-grade AAST injuries (P < 0.001). Although there was no statistically significant difference in the overall mortality (5.4% for primary repair vs. 12.5% for colostomy; P = 0.279), procedure-specific morbidity was profound. The anastomotic leak rate in the subgroup that underwent resection with primary anastomosis was 55.6%. Furthermore, stoma-related complications affected 50% of patients in the colostomy group.
Conclusion: Primary repair is the predominant strategy for treating colonic trauma in this conflicting setting, and colostomy is reserved for high-risk patients. However, our findings revealed two critical context-specific dangers: an alarming failure rate for primary anastomosis in severe injuries, and a substantial morbidity burden from stoma formation. These results suggest that when a simple primary suture is not feasible, a damage-control approach with an end colostomy may be the safest option in an austere surgical environment.
Keywords: Colonic trauma; Colostomy; Conflict surgery; Injury severity; Observational study; Primary repair; Stoma complications; Trauma.
Conflict of interest statement
Declarations. Ethical approval and consent to participate: This study was conducted in accordance with the principles of the Helsinki Declaration. The study protocol was reviewed and approved by the Institutional Review Board of Al-Thawra Modern General Hospital, Sana’a, Yemen (Reference Number: IRB-TMGH-2020-04). The requirement for written informed consent was waived, in accordance with the approval of the ethics committee. This waiver was granted owing to the prospective observational design of the study, which involved the analysis of de-identified data collected as part of routine clinical care and an established trauma registry. The study posed minimal risk to participants and did not involve any experimental interventions. Patient confidentiality was rigorously maintained throughout all phases of the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Cornwell EE, Velmahos GC, Berne TV, Murray JA, Chahwan S, Asensio J, et al. The fate of colonic suture lines in high-risk trauma patients: a prospective analysis. J Am Coll Surg. 1998;187:58–63. 10.1016/s1072-7515(98)00111-2. - PubMed
-
- Amin S, Rowlands B, Colorectal trauma. Trauma. 2000;2:211–21. 10.1177/146040860000200305.
-
- Curran TJ, Borzotta AP. Complications of primary repair of colon injury: literature review of 2,964 cases. Am J Surg. 1999;177:42–7. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
