

Global, regional, and national burden of ischemic heart disease attributable to lead exposure, 1990-2021: decomposition, frontier, and projection analysis
- PMID: 40900697
- PMCID: PMC12399670
- DOI: 10.3389/fpubh.2025.1567747
Global, regional, and national burden of ischemic heart disease attributable to lead exposure, 1990-2021: decomposition, frontier, and projection analysis
Abstract
Introduction: Ischemic heart disease (IHD) is a leading global health burden, with lead exposure identified as a significant environment risk factor contributing to its prevalence.
Methods: Data from the Global Burden of Disease Study (GBD) 2021 were used to analyze deaths and disability-adjusted life years (DALYs) of IHD due to lead exposure at global, regional, and national levels. Decomposition analysis, frontier analysis, and Bayesian age-period cohort (BAPC) models were applied to assess trends from 1990 to 2021.
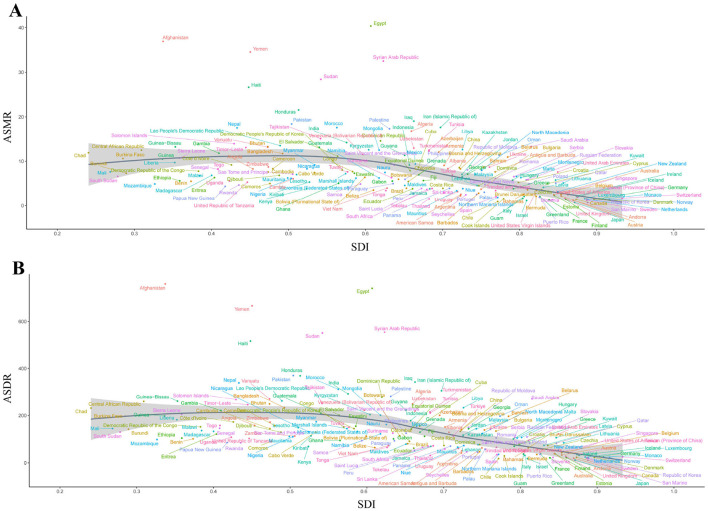
Results: In 2021, deaths and DALYs attributable to lead exposure reached 590,370.03 and 11,854,611.43, respectively, though age-standardized rates (ASRs) declined. Males and the older adult exhibited higher ASRs. At regional level, South Asia had the highest number of deaths and DALYs, while North Africa and the Middle East had the highest ASRs. Certain countries showed increasing ASRs over time, with a negative correlation between socio-demographic index (SDI) and ASRs. Decomposition analysis identified that population growth as the primary driver of increasing deaths and DALYs, particularly in middle-SDI regions. Frontier analysis suggested that middle and low-SDI regions have the greater potential to reduce the IHD burden. BAPC projections indicated a global decrease in IHD burden due to lead exposure by 2050.
Conclusions: The burden remains disproportionately high in males, the older adult and low- and middle-SDI regions, highlighting the need for targeted prevention and lead exposure control efforts in these populations.
Keywords: death; disability-adjusted life years; global burden; ischemic heart disease; lead exposure.
Copyright © 2025 Wen, Qiao, Deng, Zhou, Li, Wang, Deng, Amhare, Han and Guo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








References
-
- Collaborators GCOD. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2100–32. 10.1016/S0140-6736(24)00367-2 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical