

A machine learning algorithm to predict the success of a second microsurgical testicular sperm extraction
- PMID: 40901096
- PMCID: PMC12401292
- DOI: 10.1097/MS9.0000000000003560
A machine learning algorithm to predict the success of a second microsurgical testicular sperm extraction
Abstract
Introduction: Testicular sperm extraction (TESE) is a common procedure for retrieving sperm in men with azoospermia. However, the success rates of a second TESE following an initial unsuccessful attempt remain low. This study aims to develop and evaluate a machine learning algorithm to predict the success of a second microsurgical TESE (microTESE).
Methods: Medical records of 47 patients who underwent a second microTESE were analyzed. The dataset included variables such as procedure side, histopathology, preoperative Follicle-stimulating hormone (FSH) and testosterone levels, testicular volume, and comorbidities. Supervised machine learning algorithms, including support vector machine (SVM), were employed to predict the success of the second microTESE. The dataset was split into training (80%) and testing (20%) sets.
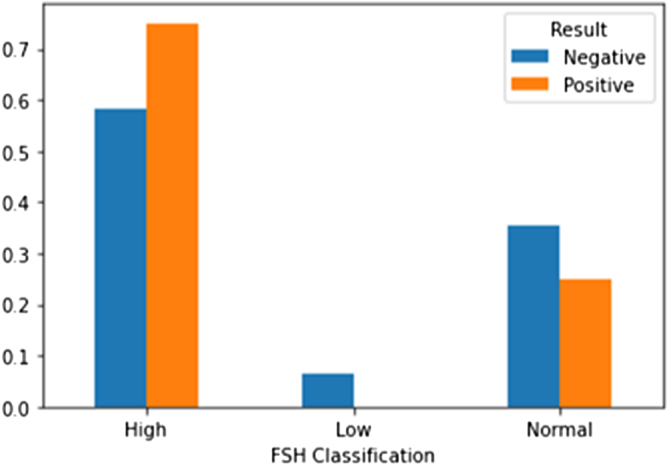
Results: The SVM model achieved an accuracy of 80% after hyperparameter tuning. Bilateral procedures and longer intervals between surgeries were associated with higher success rates, while a history of cancer correlated with negative outcomes. FSH and testosterone levels were also identified as predictive factors. The SVM model's feature importance analysis highlighted histopathology, varicocele, hormone levels, and the interval between procedures as highly correlated with the success of a second microTESE.
Discussion: The machine learning model accurately predicted the presence or absence of spermatozoa in patients with non-obstructive azoospermia undergoing a second microTESE. The findings are consistent with previous studies and provide valuable insights into the predictive factors for the success of a second microTESE. However, the study's limitations include selection bias and reliance on retrospective data.
Conclusion: The SVM model shows promise in predicting the success of a second microTESE by incorporating factors such as age, hormonal levels, testicular volume, and genetic evaluation. Further validation and refinement are needed to ensure the model's accuracy and applicability across different populations.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Can we improve time to patency with vasoepididymostomy with an innovative epididymal occlusion stitch?Int Braz J Urol. 2024 Jul-Aug;50(4):504-506. doi: 10.1590/S1677-5538.IBJU.2024.0222. Int Braz J Urol. 2024. PMID: 38743068 Free PMC article.
-
Outcome of microdissection TESE compared with conventional TESE in non-obstructive azoospermia: a systematic review.Andrology. 2014 Jan;2(1):20-4. doi: 10.1111/j.2047-2927.2013.00148.x. Epub 2013 Nov 6. Andrology. 2014. PMID: 24193894
-
Genetic determinants of testicular sperm extraction outcomes: insights from a large multicentre study of men with non-obstructive azoospermia.Hum Reprod Open. 2025 Aug 29;2025(3):hoaf049. doi: 10.1093/hropen/hoaf049. eCollection 2025. Hum Reprod Open. 2025. PMID: 40896145 Free PMC article.
-
Development of a nomogram for sperm retrieval at microTESE for idiopathic non-obstructive azoospermia in a multi-center cohort study.Andrology. 2025 Aug 29. doi: 10.1111/andr.70111. Online ahead of print. Andrology. 2025. PMID: 40884056
-
Individualised gonadotropin dose selection using markers of ovarian reserve for women undergoing in vitro fertilisation plus intracytoplasmic sperm injection (IVF/ICSI).Cochrane Database Syst Rev. 2018 Feb 1;2(2):CD012693. doi: 10.1002/14651858.CD012693.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2024 Jan 4;1:CD012693. doi: 10.1002/14651858.CD012693.pub3. PMID: 29388198 Free PMC article. Updated.
References
-
- Jarow JP, Espeland MA, Lipshultz LI. Evaluation of the azoospermic patient. J Urol 1989;142:62–65. - PubMed
-
- Ramasamy R, Schlegel PN. Microdissection testicular sperm extraction: effect of prior biopsy on success of sperm retrieval. J Urol 2007;177:1447–49. - PubMed
-
- SU LM, Palermo GD, GOLDSTEIN M, et al. Testicular sperm extraction with intracytoplasmic sperm injection for nonobstructive azoospermia: testicular histology can predict success of sperm retrieval. J Urol 1999;161:112–16. - PubMed
-
- Bernie AM, Mata DA, Ramasamy R, et al. Comparison of microdissection testicular sperm extraction, conventional testicular sperm extraction, and testicular sperm aspiration for nonobstructive azoospermia: a systematic review and meta-analysis. Fertil Steril 2015;104:1099–103. - PubMed
-
- Abdel Raheem A, Garaffa G, Rushwan N, et al. Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia. BJU Int 2013;111:492–99. - PubMed
LinkOut - more resources
Full Text Sources