

Introduction of ultrasound-guided axillary vein approach for central venous catheterization in severely injured trauma patients: characteristics and concerns
- PMID: 40901510
- PMCID: PMC12399552
- DOI: 10.3389/fmed.2025.1603778
Introduction of ultrasound-guided axillary vein approach for central venous catheterization in severely injured trauma patients: characteristics and concerns
Abstract
Background: The ultrasound-guided axillary vein approach for central venous catheterization (UAVC) demonstrates high success rates and low complications; however, its utilization in trauma care settings remains limited. This study aimed to characterize UAVC practices in a trauma intensive care unit (TICU) at a tertiary teaching hospital, specifically investigating optimal catheter positioning, procedure-related complications, and risk factors associated with catheter inaccurate placement and venous thromboembolism (VTE) development.
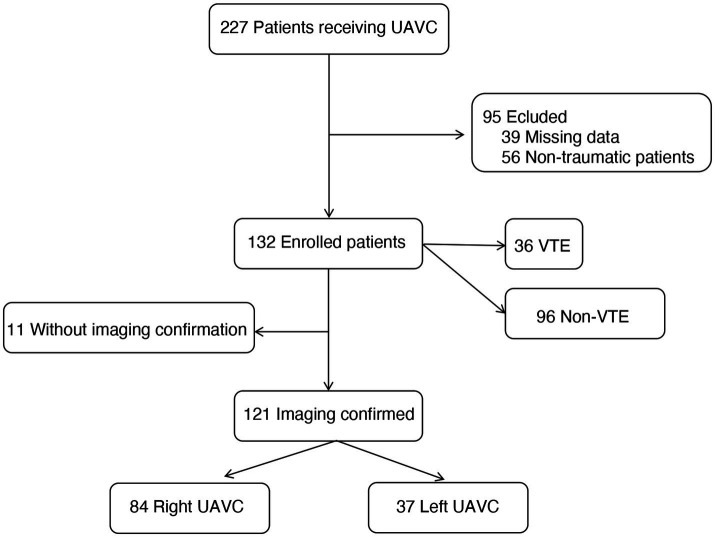
Methods: A retrospective analysis was performed on trauma patients who underwent UAVC between October 2021 and April 2023. This analysis was based on electronic medical records. Details of patients, procedures, and instances of catheter misplacement were carefully documented. The immediate complications after UAVC, including pneumothorax, hemothorax, hematoma, arteriovenous fistula, arterial dissection, and skin infection, were recorded. Moreover, late-onset complications such as VTE and catheter-related bloodstream infections (CRBSI) were also noted. Logistic regression was utilized to determine the independent risk factors for non-optimal catheter tip placement and VTE.
Results: A total of 132 UAVC cases were analyzed, with 113 (85.6%) performed by resident physicians and no immediate complications observed. The VTE incidence was 27.3%, particularly higher in elderly patients (≥ 65 years, 43.4%), and fever during TICU stay was noted in 55.3% of cases. Catheter-related infections occurred at a rate of 3.38 per 1,000 catheter days, with eight cases (6.06%) of catheter misplacement. Accurate placement was achieved in 29.8% of 121 patients, predominantly on the right side (40.4%). Factors influencing inaccurate placement included patient age [odds ratios (OR) 1.06, 95% confidence interval (CI) 1.02-1.10], obesity (OR 9.31, 95% CI 2.58-33.56), and left-side placement (OR 133.04, 95% CI 21.66-817.29), while patient age (>54 years), fever, and ventilation duration (>6.6 days) were associated with VTE development.
Conclusion: In severely injured trauma patients, UAVC is associated with a high incidence of VTE and a low rate of optimal catheter tip positioning. Our findings underscore the necessity of standardized protocols to refine catheter tip placement and warrant further investigation through randomized controlled trials.
Keywords: axillary vein; central venous catheterization; multiple trauma; ultrasound; venous thromboembolism.
Copyright © 2025 Gu, Xu, Jiang, Lu, Wang and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Venous cutdown versus the Seldinger technique for placement of totally implantable venous access ports.Cochrane Database Syst Rev. 2016 Aug 21;2016(8):CD008942. doi: 10.1002/14651858.CD008942.pub2. Cochrane Database Syst Rev. 2016. PMID: 27544827 Free PMC article.
-
Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization.Cochrane Database Syst Rev. 2015 Jan 9;1(1):CD011447. doi: 10.1002/14651858.CD011447. Cochrane Database Syst Rev. 2015. PMID: 25575245 Free PMC article.
-
Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization.Cochrane Database Syst Rev. 2015 Jan 9;1(1):CD006962. doi: 10.1002/14651858.CD006962.pub2. Cochrane Database Syst Rev. 2015. PMID: 25575244 Free PMC article.
-
Interventions for treating catheter-related bloodstream infections in people receiving maintenance haemodialysis.Cochrane Database Syst Rev. 2022 Apr 1;4(4):CD013554. doi: 10.1002/14651858.CD013554.pub2. Cochrane Database Syst Rev. 2022. PMID: 35363884 Free PMC article.
-
Catheter impregnation, coating or bonding for reducing central venous catheter-related infections in adults.Cochrane Database Syst Rev. 2016 Mar 16;3(3):CD007878. doi: 10.1002/14651858.CD007878.pub3. Cochrane Database Syst Rev. 2016. PMID: 26982376 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous