

Impact of the absence of opioid anesthesia on postoperative outcome indicators: a systematic review and meta-analysis
- PMID: 40901514
- PMCID: PMC12399677
- DOI: 10.3389/fmed.2025.1639968
Impact of the absence of opioid anesthesia on postoperative outcome indicators: a systematic review and meta-analysis
Abstract
Objective: This study aimed to examine the effect of opioid-free anesthesia (OFA) on postoperative outcome indicators and explore its application in thoracoscopic or laparoscopic as well as non-thoracoscopic or laparoscopic surgeries, providing a scientific basis for clinical decision-making.
Method: A systematic search was conducted for clinical studies comparing OFA and opioid-based anesthesia (OBA) published from the establishment of the databases to May 2025 using databases such as PubMed, Web of Science, Embase, and Cochrane Library. The primary outcome was the incidence of postoperative nausea and vomiting (PONV). Secondary outcomes included perioperative recovery indicators, the need for postoperative emergency analgesia, postoperative pain score (VAS, NRS), and adverse reactions.
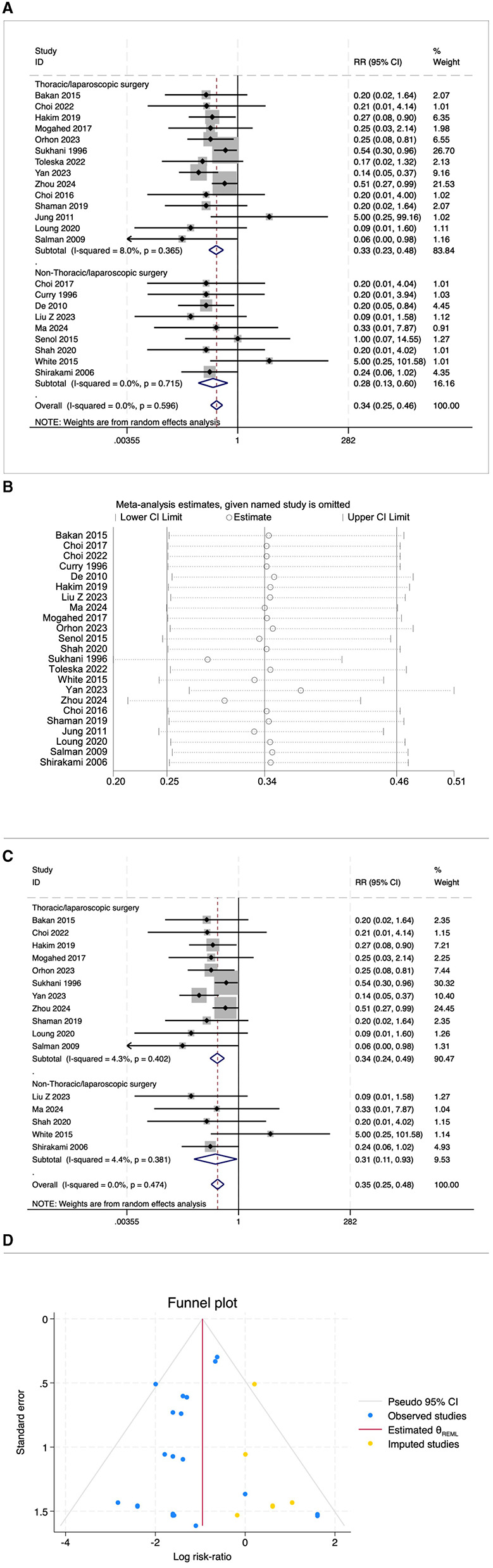
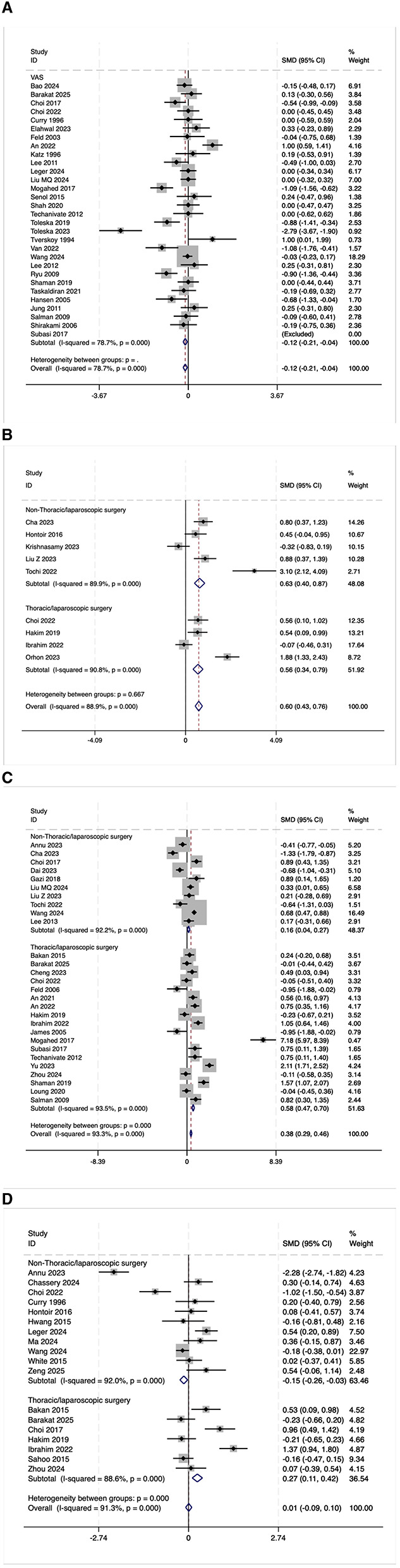
Results: A total of 3,766 relevant studies were initially identified, and 68 randomized controlled trials involving 5,426 patients were ultimately included. Compared with OBA, OFA significantly reduced the risks of PONV (RR = 0.50, 95% CI: 0.39-0.64), nausea alone (RR = 0.34, 95% CI: 0.25-0.46), vomiting alone (RR = 0.34, 95% CI: 0.25-0.46), and the need for postoperative emergency analgesia (RR = 0.61, 95% CI: 0.51-0.72). OFA was also associated with lower 24 h postoperative NRS pain scores (SMD = -0.32, 95% CI: -0.53 to -0.10). For outcomes with high heterogeneity (I 2 > 75%), the systematic review showed that most studies did not find a significant reduction in postoperative VAS pain scores with OFA. However, over two-thirds of the studies have shown that OFA can improve the quality of postoperative recovery (QoR-40). Approximately half of the studies suggested that OFA may prolong extubation time, while most found no significant difference in PACU stay time.
Conclusion: In summary, OFA not only significantly reduces postoperative PONV, but also lowers the demand for analgesic drugs and improves the quality of postoperative recovery. However, its effect on some postoperative recovery indicators is limited, and further high-quality studies are required to confirm these findings. OFA is expected to serve as a safe and effective anesthesia strategy to optimize the perioperative outcomes of patients.
Keywords: meta-analysis; opioid drugs; opioid-free anesthesia; postoperative recovery; systematic review.
Copyright © 2025 Qin, Zhang, Bo, Ma and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Opioid-Free Anesthesia Improved the Quality of Recovery After Thyroidectomy Through Pre-Emptive and Preventive Analgesia: A Randomized Controlled Trial.Drug Des Devel Ther. 2025 Jun 19;19:5243-5254. doi: 10.2147/DDDT.S520856. eCollection 2025. Drug Des Devel Ther. 2025. PMID: 40552090 Free PMC article. Clinical Trial.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Effect of Opioid-Free Versus Opioid Anesthesia on the Quality of Postoperative Recovery in Patients Receiving Laparoscopic Sleeve Gastrectomy.Obes Surg. 2025 Aug;35(8):3120-3130. doi: 10.1007/s11695-025-08008-y. Epub 2025 Jun 25. Obes Surg. 2025. PMID: 40555931 Free PMC article. Clinical Trial.
-
Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults.Cochrane Database Syst Rev. 2018 Jun 4;6(6):CD009642. doi: 10.1002/14651858.CD009642.pub3. Cochrane Database Syst Rev. 2018. PMID: 29864216 Free PMC article.
References
-
- Bao R, Zhang WS, Zha YF, Zhao ZZ, Huang J, Li JL, et al. Effects of opioid-free anaesthesia compared with balanced general anaesthesia on nausea and vomiting after video-assisted thoracoscopic surgery: a single-centre randomised controlled trial. BMJ Open. (2024) 14:e079544. 10.1136/bmjopen-2023-079544 - DOI - PMC - PubMed
-
- Beloeil H, Laviolle B, Menard C, Paugam-Burtz C, Garot M, Asehnoune K, et al. SFAR research network. POFA trial study protocol: a multicentre, double-blind, randomised, controlled clinical trial comparing opioid-free versus opioid anaesthesia on postoperative opioid-related adverse events after major or intermediate non-cardiac surgery. BMJ Open. (2018) 8:e020873. 10.1136/bmjopen-2017-020873 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources