

Dynamic nomogram predicts sepsis risk in patients with acute liver failure: Analysis of intensive care database with external validation
- PMID: 40901690
- PMCID: PMC12400238
- DOI: 10.3748/wjg.v31.i31.105229
Dynamic nomogram predicts sepsis risk in patients with acute liver failure: Analysis of intensive care database with external validation
Abstract
Background: Acute liver failure (ALF) with sepsis is associated with rapid disease progression and high mortality. Therefore, early detection of high-risk sepsis subgroups in patients with ALF is crucial.
Aim: To develop and validate an accurate nomogram model for predicting the risk of sepsis in patients with ALF.
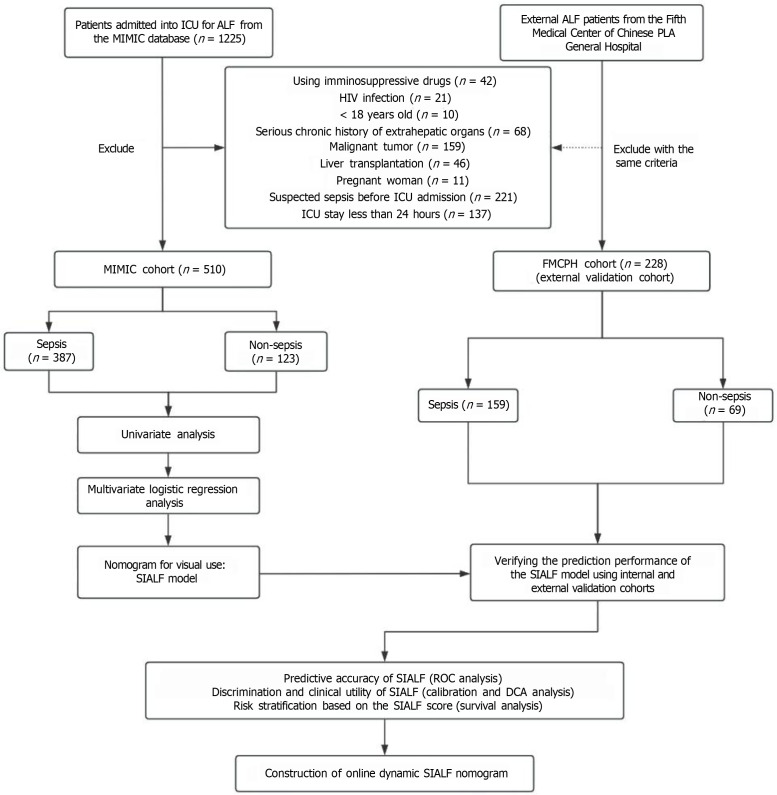
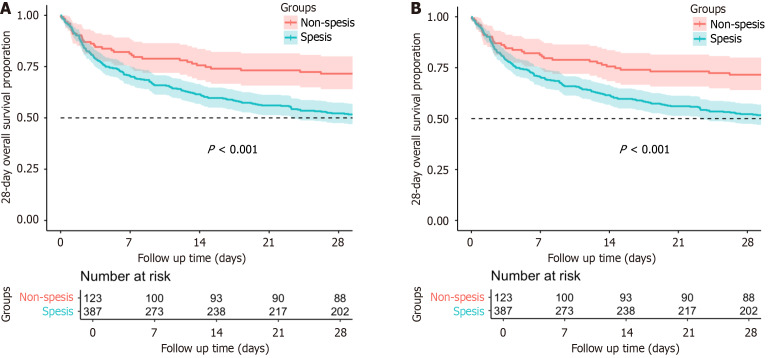
Methods: We retrieved data from the Medical Information Mart for Intensive Care (MIMIC) IV database and the Fifth Medical Center of Chinese PLA General Hospital (FMCPH). Univariate and multivariate logistic regression analysis were used to identify risk factors for sepsis in ALF and were subsequently incorporated to construct a nomogram model [sepsis in ALF (SIALF)]. The discrimination ability, calibration, and clinical applicability of the SIALF model were evaluated by the area under receiver operating characteristic curve, calibration curves, and decision curve analysis, respectively. The Kaplan-Meier curves were used for robustness check. The SIALF model was internally validated using the bootstrapping method with the MIMIC validation cohort and externally validated by the FMCPH cohort.
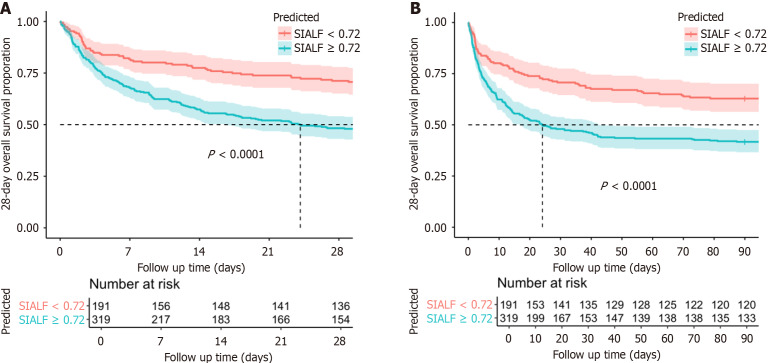
Results: A total of 738 patients with ALF patients were included in this study, with 510 from the MIMIC IV database and 228 from the FMCPH cohort. In the MIMIC IV cohort, 387 (75.89%) patients developed sepsis. Multivariate logistic regression analysis revealed that age [odds ratio (OR) = 1.016, 95% confidence interval (CI): 1.003-1.028, P = 0.017], total bilirubin (OR = 1.047, 95%CI: 1.008-1.088, P = 0.017), lactate dehydrogenase (OR = 1.001, 95%CI: 1.000-1.001, P < 0.001), albumin (OR = 0.436, 95%CI: 0.274-0.692, P = 0.003), and mechanical ventilation (OR = 1.985, 95%CI: 1.269-3.105, P = 0.003) were independent risk factors associated with sepsis in patients with ALF. The SIALF model demonstrated satisfactory accuracy and clinical utility with area under receiver operating characteristic curve values of 0.849, 0.847, and 0.835 for the internal derivation, internal validation, and external validation cohort, respectively, which outperformed the Sequential Organ Failure Assessment scores of 0.733, 0.746, and 0.721 and systemic inflammatory response syndrome scores of 0.578, 0.653, and 0.615, respectively. The decision curve analysis and calibration curves indicated superior clinical utility and efficiency than other score systems. Based on the risk stratification score derived from the SIALF model, the Kaplan-Meier curves effectively discriminated the real high-risk subpopulation. To enhance the clinical utility, we constructed an online dynamic version, enabling physicians to evaluate patients' condition and track disease progression in real-time.
Conclusion: Based on easily identifiable clinical data, we developed the SIALF model to predict the risk of sepsis in patients with ALF. The model demonstrated robust predictive efficiency, outperformed Sequential Organ Failure Assessment and systemic inflammatory response syndrome scores, and was validated in an external cohort. The model-based risk stratification and online calculator might further facilitate the early detection and appropriate treatment for this subpopulation.
Keywords: Acute liver failure; Nomogram; Predict; Risk stratification; Sepsis.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors report no relevant conflicts of interest for this article.
Figures




References
-
- Polson J, Lee WM American Association for the Study of Liver Disease. AASLD position paper: the management of acute liver failure. Hepatology. 2005;41:1179–1197. - PubMed
-
- MacDonald AJ, Speiser JL, Ganger DR, Nilles KM, Orandi BJ, Larson AM, Lee WM, Karvellas CJ US Acute Liver Failure Study Group. Clinical and Neurologic Outcomes in Acetaminophen-Induced Acute Liver Failure: A 21-Year Multicenter Cohort Study. Clin Gastroenterol Hepatol. 2021;19:2615–2625.e3. - PMC - PubMed
-
- Strnad P, Tacke F, Koch A, Trautwein C. Liver - guardian, modifier and target of sepsis. Nat Rev Gastroenterol Hepatol. 2017;14:55–66. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
