

Large-scale online assessment uncovers a distinct Multiple Sclerosis subtype with selective cognitive impairment
- PMID: 40903471
- PMCID: PMC12408825
- DOI: 10.1038/s41467-025-62156-4
Large-scale online assessment uncovers a distinct Multiple Sclerosis subtype with selective cognitive impairment
Abstract
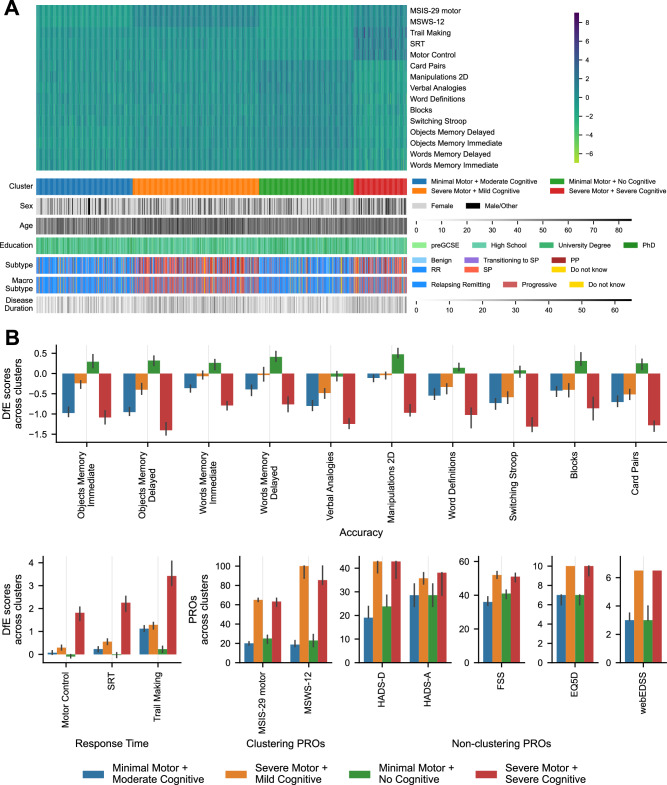
Cognitive impairments in Multiple Sclerosis (MS) are prevalent and disabling yet often unaddressed. Here, we optimised automated online assessment technology for people with MS and used it to characterise their cognitive deficits in greater detail and at a larger population scale than previously possible. The study involved 4526 UK MS Register members over three stages. Stage 1 evaluated 22 online cognitive tasks and established their feasibility. Based on MS discriminability a 12-task battery was selected. Stage 2 validated the resulting battery at scale, while Stage 3 compared it to a standard neuropsychological assessment. Clustering analysis identified a prevalent MS subtype exhibiting significant cognitive deficits with minimal motor impairment. Disability in this group is currently unrecognised and untreated. These findings underscore the importance of cognitive assessment in MS, the feasibility of integrating online tools into patient registries, and the potential of such large-scale data to derive insights into symptom heterogeneity.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.H. is the founder and director of Future Cognition Ltd and co-founder and co-director of H2CD, which develops custom online assessment software and provides online assessment technology as a service for third parties, primarily in the research and healthcare sectors. P.J.H. is co-founder and co-director of H2CD. W.T. works as an employee of H2CD. R.N. has carried out paid advisory board and research trial with Roche and Novartis. He is vice chair of the National Institute for Health and Care Excellence HTA committee C. E.CO has received honoraria for consultancy or speaking from Biogen, Novartis, Sanofi, Merck, Roche, Bristol, Janssen, and Alexion. All other authors report no competing interests.
Figures





References
-
- Chiaravalloti, N. D. & DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol.7, 1139–1151 (2008). - PubMed
-
- Rao, S. M., Leo, G. J., Bernardin, L. & Unverzagt, F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology41, 685–691 (1991). - PubMed
-
- Khalil, M. et al. Cognitive impairment in relation to MRI metrics in patients with clinically isolated syndrome. Mult. Scler. J.17, 173–180 (2011). - PubMed
-
- Amato, M. P. et al. Neuropsychological features in childhood and juvenile multiple sclerosis: five-year follow-up. Neurology83, 1432–1438 (2014). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
